Compiled from clinical pathology references. Medically reviewed by Dr Cristian Dunker , Principal Dentist, ArtSmiles Cosmetic Dentistry.
Quick summary
Also called | Acute apical abscess (a collection of pus walled off from surrounding tissue), dento-alveolar abscess, acute apical periodontitis with suppuration, symptomatic apical abscess |
How urgent? | 🔴 See a dentist promptly, a periapical (at the tip of a tooth root) abscess is an active infection at the root tip of a dead tooth and can spread into nearby tissues if it is left untreated. |
Common or rare? | Very common, one of the most frequent reasons people present to a dentist with severe toothache. |
Who it affects | Adults and children. Anyone with a deeply decayed, heavily restored, cracked, or previously injured tooth is at risk. |
Who treats it | A general dentist can usually manage it. Specialist endodontic referral may be considered for complex root canal anatomy or persistent infection. |
Based on | Regezi, Neville, and Cawson |
What is it?
A periapical abscess is a pocket of pus that forms in the bone right at the very tip of a tooth root. It develops when the nerve and blood supply inside the tooth (the pulp), the soft nerve and blood vessel core of the tooth has died and bacteria have travelled out of the root canal into the surrounding bone. The result is a localised acute infection that is usually painful, often dramatically so, and that signals the body is trying to wall off and fight the infection at the end of the root.
Who tends to get it?
Periapical abscesses can occur at any age and in any tooth. They show up most often in adults who have a long history of dental work, deep cavities, or a previous knock to a front tooth, but children with untreated decay in baby teeth or first permanent molars are also commonly affected.
The textbooks describe no strong sex or ethnic bias. The single biggest risk factor is simply having a tooth in which the nerve has died, and that can happen to anyone. The lower back teeth, the upper front teeth, and any tooth with a large filling, a crown, or a previous root canal are particularly prone.
What causes it?
The overwhelming cause is bacterial infection that reaches the pulp and kills it. The most common pathway is dental decay (caries) that has worked its way through the enamel and dentine and into the pulp chamber. Once bacteria contaminate the pulp, the inflammation that follows often cannot resolve, the pulp dies, and the infection then drains out of the root tip into the surrounding bone.
Other recognised triggers include:
Deep fillings or crown preparations that have irritated the pulp over time, even without active decay
Trauma, a blow to a tooth that damages the apical blood vessels and quietly kills the pulp, sometimes years before the abscess appears
A cracked or fractured tooth that allows bacteria a direct route into the pulp
Severe gum disease that has tracked along the root and entered through a side canal
Previous root canal treatment in which a small amount of infection has remained or re-entered the canal system
The bacteria involved are typically a mixed group of organisms that normally live in the mouth, dominated by anaerobes (bacteria that thrive without oxygen). Modern molecular studies have shown the mix is far more diverse than older culture techniques suggested.
How does it develop?
Think of a tooth as a small living organ encased in hard, unyielding shell. Inside that shell sits the pulp, a delicate package of nerves and blood vessels. When bacteria reach the pulp, the body tries to fight back with inflammation. But because the pulp is sealed inside the tooth, there is nowhere for the swelling to go. Pressure builds, the blood supply is cut off, and the pulp dies.
Once the pulp is dead, bacteria and their toxins seep out through the tiny opening at the root tip into the bone beyond. The bone responds in one of two ways. If the infection is slow and low-grade, the body forms a chronic lesion (a periapical granuloma or cyst) that can sit there quietly for years. If the infection is fast or aggressive, neutrophils, the body's emergency-response white blood cells, flood in and create pus. That pocket of pus is the periapical abscess.
The abscess can also flare up suddenly out of a long-standing chronic lesion. When that happens, dentists call it a phoenix abscess, named after the mythical bird that rises from its own ashes, a once-quiet granuloma that has erupted back into acute infection.
What might you notice?
What it looks like
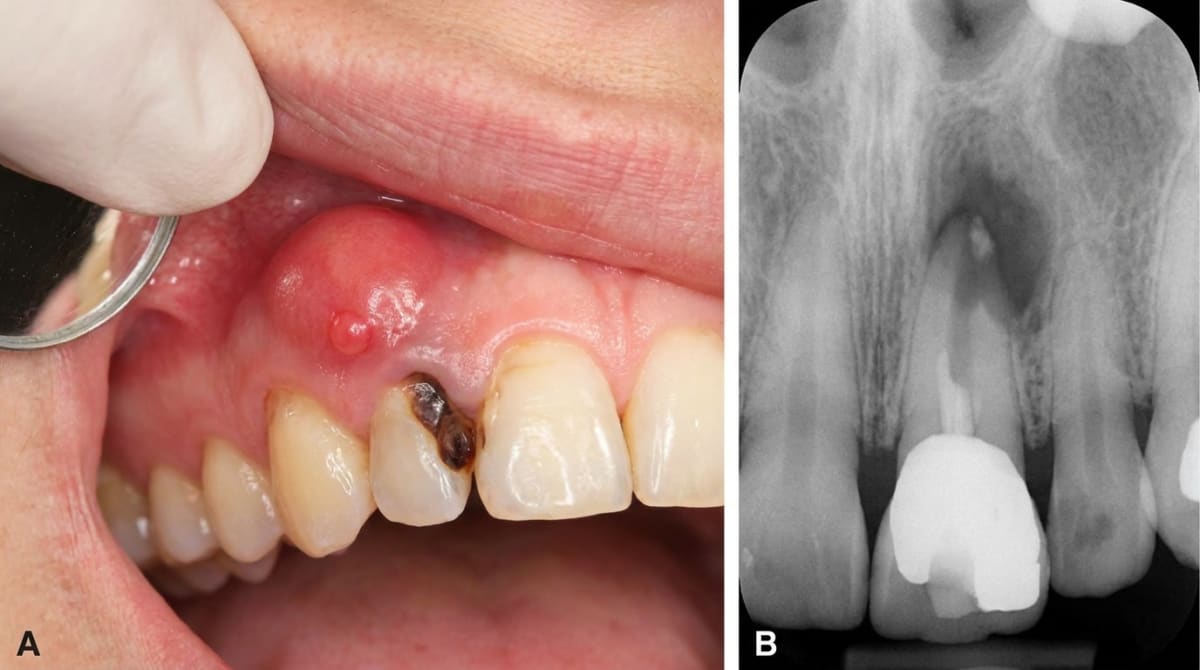
In the earliest stage there may be nothing visible at all, the trouble is hidden inside the bone. As pressure builds, the gum over the root may become red, shiny, and tender. A swelling can appear in the cheek, lip, palate, or under the jaw. Sometimes the body finds its own drainage route and a small pimple-like bump (a parulis or gum boil) appears on the gum, often releasing a salty taste of pus. The tooth itself may look discoloured, grey, brown, or yellowed, because the pulp inside has died.
What it feels like
The classic story is severe, constant, throbbing pain in one specific tooth. Unlike pain from a sensitive or inflamed pulp, pain from a periapical abscess is usually easy to localise, most people can point straight to the offending tooth. The tooth often feels high in the bite, as if it has grown a little proud of its neighbours, and even gentle touch with the tongue or a slight tap may be excruciating. Hot or cold no longer trigger sharp pain because the nerve is already dead. Headache, malaise, fever, chills, and tender lymph nodes under the jaw or neck can develop as the body mounts a wider response.
If the pus finds a way out, through a gum boil or sinus tract (a small drainage channel from a deep infection to the gum or skin), the pressure drops and the pain often eases dramatically. That feeling of relief is misleading; the underlying infection is still there.
What an X-ray might show
In the very early stages, an X-ray may look surprisingly normal because the abscess has not had time to dissolve any bone. The first subtle change is usually a slight widening of the dark line around the root tip (the periodontal ligament space) and a hazy lamina dura, the thin sheet of bone lining the socket. With more time, an ill-defined dark area (radiolucency) develops at the root tip. A phoenix abscess sits on top of an already established round dark area from the chronic lesion that came before it. cone-beam CT (a 3D dental X-ray) scans can give a more detailed picture when needed.
What happens at the dentist?
At ArtSmiles, diagnosis usually begins with a careful conversation about the pain, when it started, what triggers it, and whether the tooth has had previous trouble. Your dentist will then examine the area and run some simple chair-side tests:
Percussion test, gently tapping the tooth. A periapical abscess is typically exquisitely tender to even light tapping.
Pulp vitality testing, a cold spray or a small electrical stimulus to check whether the nerve is alive. A tooth with a periapical abscess does not respond, because the pulp is dead.
Palpation of the gum and surrounding tissues for swelling or fluctuance (a soft, fluid-filled feel).
Periapical X-ray of the tooth, and sometimes a cone-beam CT scan if the picture is unclear or the anatomy is complex.
If a sinus tract is present, your dentist may carefully thread a small flexible point (a gutta-percha point) into the opening and take an X-ray. The point follows the channel back to the source tooth, which is not always the one you would expect.
Most periapical abscesses can be diagnosed and managed in a general dental setting. Specialist referral to an endodontist (a dentist who specialises in root canal treatment) may be considered for teeth with complex root canal anatomy, persistent infection after previous treatment, or unusual radiographic findings that need further investigation.
Is this serious?
🔴 A periapical abscess should be treated promptly. While a well-localised abscess in a healthy patient is rarely life-threatening, a dental infection has the potential to spread along the soft-tissue planes of the face and neck. When it does, it can cause dental abscess and cellulitis (a spreading bacterial infection through the soft tissues), and in rare cases serious complications such as Ludwig's angina (a dangerous swelling under the tongue and jaw) or cavernous sinus thrombosis. People with diabetes, weakened immune systems, or other significant medical conditions are at higher risk of these complications.
The good news is that once drainage is established and the infection is treated, the bone usually heals well and the outlook is excellent.
If you have severe toothache, swelling of the face, fever, difficulty swallowing, or trouble opening your mouth, it's worth booking an urgent assessment.
Could it be something else?
Several other conditions can cause similar pain or swelling. The dentist's job is to work out which one is the real culprit.
Periapical granuloma, the chronic, slow-burning version of the same disease. It can look identical on an X-ray as a dark area at the root tip, but it is usually painless. The dentist tells them apart by symptoms (granuloma is quiet, abscess is painful and tender to percussion).
Periapical cyst (radicular cyst), a fluid-filled sac that can grow from a long-standing granuloma. Also typically painless and discovered on routine X-ray; differentiated by its larger, well-defined, often round dark area on imaging and confirmed by histology after removal.
Periodontal abscess, a pus pocket in the gum rather than at the root tip, arising from gum disease. The tooth is usually still alive (responds to vitality testing), there is a deep gum pocket, and the swelling is closer to the gum line rather than over the root apex.
Vertical root fracture, a crack down the length of the root that lets bacteria in. Often presents with similar pain and swelling but typically shows a narrow, J-shaped radiolucency along the side of the root and a deep, isolated, narrow gum pocket.
Acute (irreversible) pulpitis without abscess, the tooth nerve is severely inflamed but has not yet died. Pain is severe but usually triggered by hot, cold, or sweet, the tooth still responds to vitality testing, and it is not yet tender to percussion.
Acute apical periodontitis from trauma or a high filling, inflammation around the root tip without infection, caused by a recent biting injury or an over-tall restoration. The tooth is usually still vital, and adjusting the bite often resolves it quickly.
Maxillary sinusitis, inflammation of the sinus above the upper back teeth can mimic toothache. Multiple upper teeth are tender, the teeth all test vital, and there are usually nasal symptoms (blocked or runny nose, pressure on bending forward).
Acute osteomyelitis of the jaw, infection of the bone itself, often a complication of an untreated abscess. Pain, swelling, and fever are more diffuse, and there may be numbness of the lower lip if the mandible is involved.
Cracked tooth, a fine crack through the crown that triggers sharp pain on biting and release. Pain is provoked rather than constant, and the tooth usually still responds to vitality testing.
How is it treated?
The two priorities are to drain the pus and to eliminate the source of infection. Both have to happen for the abscess to resolve properly.
What you can do at home before your appointment:
Take simple analgesics such as paracetamol or ibuprofen at the recommended dose if you are able to, the textbooks note that anti-inflammatory pain relief is usually appropriate before, during, and after treatment.
Keep the area clean with gentle warm salt-water rinses.
Try to keep the tooth out of the bite where possible.
Avoid applying heat to the face, warm compresses can sometimes encourage swelling to spread.
See a dentist promptly. Painkillers and rinses do not treat the underlying infection.
Professional treatment may include:
Drainage through the tooth, opening the tooth and clearing the canal lets pus escape from the root tip and immediately relieves pressure. This is often the single most effective step for pain relief.
Incisional drainage, if there is a fluctuant swelling in the gum or face, the dentist may numb the area and make a small incision to release the pus. Drainage through both the tooth and the soft tissue is sometimes needed.
Reducing the bite, if the tooth is sitting high, gently grinding the surface a fraction can stop ongoing trauma and help the inflammation settle.
Definitive treatment of the source, once the acute infection is under control, the tooth needs either:
Root canal treatment to remove the dead pulp tissue, disinfect the canal system, and seal it; or
Extraction of the tooth if it is not restorable.
Antibiotics, the textbooks are clear that antibiotics are not routinely required for a well-localised abscess in a healthy person who has had drainage. They are reserved for patients with signs of spreading infection (significant swelling, cellulitis, fever, swollen lymph nodes, malaise), patients who are medically compromised, or situations where definitive dental care is delayed.
Specialist referral to an endodontist may be considered for complex cases, persistent infection, or teeth that have failed previous root canal treatment. An oral surgeon may be involved if a more challenging extraction or surgical drainage is needed.
With good drainage and definitive treatment, the textbooks note that signs and symptoms typically diminish significantly within 48 hours.
What's the long-term outlook?
The outlook for a periapical abscess that is treated promptly is generally very good. Once the source of infection is dealt with, through root canal treatment or extraction, the bone around the root tip usually heals over the following months and the radiolucent area on the X-ray slowly fills back in.
A tooth that has had a successful root canal can give many years of good service if properly restored, often with a crown, to protect what remains of the natural structure. Where a tooth has been extracted, options to replace it include a dental implant, a bridge, or a denture, depending on the wider clinical picture.
Sinus tracts (gum boils) typically heal on their own within a few weeks of the underlying infection being resolved. Occasionally a tract that has been there a long time needs minor surgical removal for it to settle completely.
The key message is that a periapical abscess is essentially a tooth that is signalling for help. With timely, appropriate care it is a manageable and resolvable problem, and the earlier it is treated, the simpler the treatment is likely to be.
A note on this article
This article is for educational purposes only and does not constitute a clinical diagnosis. Please consult a registered dental practitioner for assessment and treatment advice.
The cover image above is an AI-generated illustration based on the most common visible features of this condition described in clinical pathology references. It is not a photograph of a real case and should not be used to diagnose or rule out the condition in your own situation. If you are concerned about something you have noticed, please book an assessment with a registered dental practitioner.
References
Regezi, J. A., Sciubba, J. J., & Jordan, R. C. K. (2017). Oral pathology: Clinical pathologic correlations (7th ed.). Elsevier. Chapter 13, Inflammatory Jaw Lesions: Periapical Abscess, pp. 313 to 317.
Neville, B. W., Damm, D. D., Allen, C. M., & Chi, A. C. (2023). Oral and maxillofacial pathology (5th ed.). Elsevier. Chapter 3, Pulpal and Periapical Disease: Periapical Abscess, pp. 129 to 132.
Cawson, R. A., & Odell, E. W. (2017). Cawson's essentials of oral pathology and oral medicine (8th ed.). Elsevier. Chapter 4, Pulpitis, Apical Periodontitis, Resorption and Hypercementosis: Acute Apical Periodontitis and Chronic Apical Periodontitis, pp. 65 to 69.
Frequently asked questions
What is the difference between a periapical abscess and a periodontal abscess?
A periapical abscess starts at the tip of the tooth root from an infected pulp (usually caused by deep decay or trauma). A periodontal abscess starts in the gum pocket from gum disease. They can look similar from the outside, but the cause and treatment differ: a periapical abscess needs root canal treatment or extraction, a periodontal abscess needs gum treatment.
Can a periapical abscess heal on its own?
No. Even if the swelling and pain settle for a while after the abscess drains, the underlying infected pulp tissue remains. Without treatment, the infection can spread into the bone, the face, or, rarely, more distant body sites. Definitive care of the source tooth is essential.
Will I need a root canal or extraction?
That depends on whether the tooth is restorable and on your overall plan. Root canal treatment removes the infected pulp and saves the natural tooth. Extraction removes the source of infection if the tooth is broken down, cracked or has a poor long-term outlook. Your dentist will discuss both options.
When is a periapical abscess an emergency?
If swelling is spreading across the face or down the neck, if you have a fever or feel unwell, if it is hard to swallow, breathe, or open your mouth, treat that as a medical emergency and seek urgent care. Most localised periapical abscesses can be managed by a dentist within 24-48 hours.



