Compiled from clinical pathology references. Medically reviewed by Dr Cristian Dunker, Principal Dentist, ArtSmiles Cosmetic Dentistry.
Ludwig's angina is a rare but serious infection of the spaces under the jaw and tongue. It is named after the nineteenth-century German physician Wilhelm Friedrich von Ludwig, who first described it. While much less common than it once was, it remains a true dental emergency because of its potential to obstruct the airway.
This article from the team at ArtSmiles, reviewed by Dr Cristian Dunker, explains what Ludwig's angina is and why it must always be taken seriously.
Important. Suspected Ludwig's angina is a medical emergency. If you have rapidly spreading swelling under your jaw, difficulty breathing or swallowing, please go to the nearest hospital emergency department immediately.
What is it?
Ludwig's angina is a rapidly progressive bacterial cellulitis (a rapidly spreading bacterial infection in soft tissue) that involves three connected spaces in the floor of the mouth and neck, the submandibular (under the jaw), sublingual (under the tongue) and submental (under the chin) spaces. The infection is usually bilateral, affecting both sides, and tends to push the tongue and floor of the mouth upwards and backwards, narrowing the airway.
Common features include:
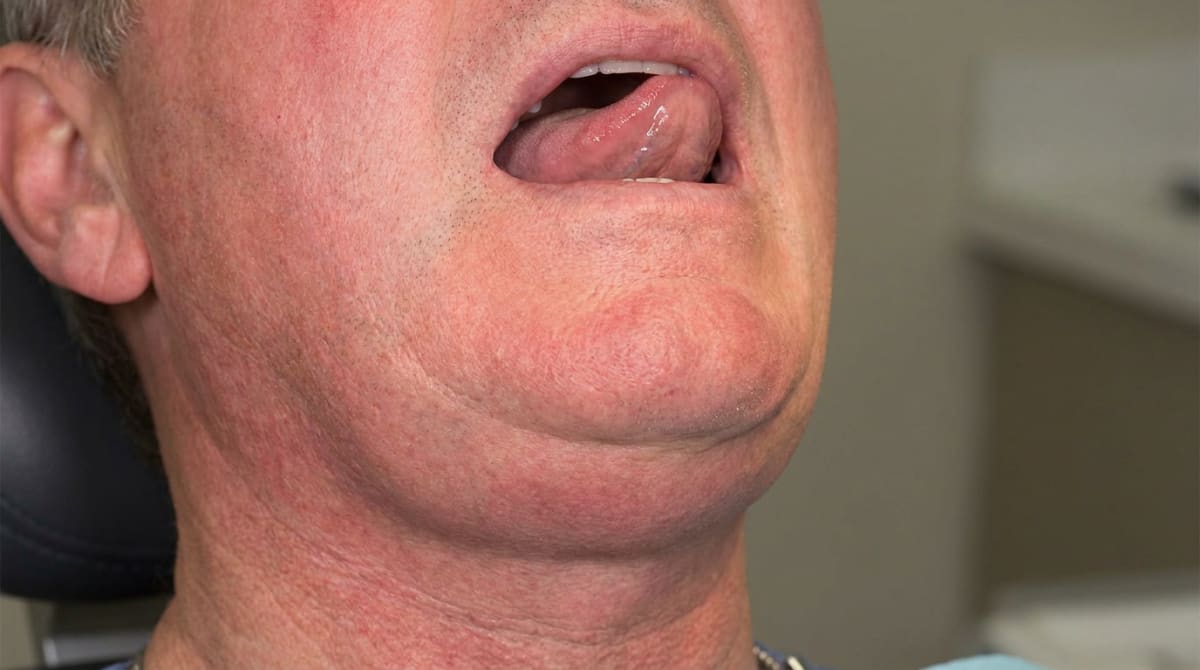
Bilateral hard swelling under the jaw.
A "woody" feeling of the floor of the mouth on examination.
Tongue elevation with the tongue pressed against the palate.
Severe pain and trismus (limited mouth opening).
Drooling because of difficulty swallowing.
Hot potato voice, muffled, thick speech.
Difficulty breathing as the airway narrows.
Fever, chills and feeling severely unwell.
Tachycardia (fast heart rate) and dehydration from severe illness.
Who tends to get it?
Ludwig's angina is most often seen in:
Adults aged 20 to 60.
Patients with an untreated lower molar infection, usually a second or third molar.
Patients with poor oral health.
Patients with diabetes, alcoholism or immunosuppression.
Patients after dental procedures in some cases.
Children, less commonly than adults.
What causes it?
The condition is bacterial. The most common source is a deep infection from a lower molar tooth, particularly the second molar, whose roots sit close to the floor-of-mouth space. Other sources include:
Periodontal abscesses of lower teeth.
Pericoronitis of an erupting wisdom tooth.
Submandibular salivary gland infection.
Mouth lacerations or facial fractures.
Recent dental injections in rare cases.
The bacteria are usually a mixed population of streptococci, staphylococci and oral anaerobes.
How does it develop?
The course is rapid:
A lower tooth becomes severely infected.
The infection spreads through the bone and into the soft tissues of the floor of mouth.
Within hours, the swelling crosses the midline and involves both sides.
The tongue is pushed upwards and backwards.
The airway narrows, breathing becomes difficult.
Without prompt treatment, the patient may suffocate.
Spread to the deeper neck spaces and chest can be fatal.
What might you notice?
Early features include:
Severe lower toothache in the days before.
A swelling under one side of the jaw that quickly spreads to both sides.
A firm, painful, unyielding feel to the floor of the mouth.
Difficulty opening the mouth.
Trouble swallowing, then drooling.
A muffled voice.
Fever and feeling severely unwell.
Tongue elevation visible in the mirror.
Increasing breathing difficulty, a sign the airway is becoming compromised.
What happens at the dentist?
Ludwig's angina is not managed at a dental practice, it is hospital-based care. The dental role is:
Recognising the picture quickly.
Calling an ambulance or directing the patient to the emergency department.
Maintaining the airway until help arrives, sitting upright, leaning forward.
Providing the hospital with the dental history, which tooth, how long, any procedures.
Following up for the source tooth treatment after the acute phase.
If you have any of these features, do not delay to attend a routine dental appointment. Go directly to the hospital emergency department.
Is this serious?
Ludwig's angina is life-threatening because:
The airway can close as the floor of mouth swells.
Infection can spread to the deep neck spaces and chest.
Septic shock can develop in severe cases.
Even with modern care, mortality is around 8%, and was much higher before antibiotics.
With prompt hospital care, however, most patients recover fully.
Could it be something else?
Conditions that can produce facial or neck swelling include:
Submandibular salivary gland infection without spread.
Submandibular abscess confined to one side.
Severe Quincke (angio-oedema) allergic swelling, usually itchy and rapid, without infection signs.
Severe pharyngitis (throat inflammation) or peritonsillar abscess (a pus collection beside a tonsil), pain in throat, deviation of uvula.
Mumps, bilateral parotid (in front of the ear) swelling, not under the jaw.
Tumours of the floor of mouth or salivary glands, usually slower in onset.
The key features distinguishing Ludwig's angina are rapid bilateral progression, woody floor of mouth and airway threat.
How is it treated?
Treatment is hospital-based, urgent and aggressive:
Airway management, the most critical step. Many patients need fibreoptic intubation (passing a breathing tube guided by a tiny camera) or emergency tracheostomy (an emergency opening made in the windpipe so the patient can breathe).
Intravenous antibiotics, typically broad-spectrum cover including against anaerobes (penicillin plus metronidazole, or a similar combination).
Surgical drainage of the infected spaces, performed by an oral and maxillofacial surgeon or ENT surgeon.
Removal of the source tooth during or after the acute phase.
Intravenous fluids and supportive care.
Intensive care in significant cases.
What's the long-term outlook?
With early hospital care, most patients recover fully within one to two weeks. Late presentation, particularly with airway compromise before hospital arrival, is associated with much higher mortality.
The single most important preventive measure is prompt treatment of dental infection. A nagging toothache that has been ignored for weeks is the most common starting point. Please do not put off dental care for a painful or swollen tooth, booking an appointment early is the simplest way to avoid this kind of emergency.
If you have noticed rapid swelling under your jaw, difficulty swallowing or any breathing trouble, please go to your nearest hospital emergency department immediately.
A note on this article
This article is for educational purposes only and does not constitute a clinical diagnosis. Please consult a registered dental practitioner for assessment and treatment advice.
The cover image above is an AI-generated illustration based on the most common visible features of this condition described in clinical pathology references. It is not a photograph of a real case and should not be used to diagnose or rule out the condition in your own situation. If you are concerned about something you have noticed, please book an assessment with a registered dental practitioner.
References
Neville, B. W., Damm, D. D., Allen, C. M., & Chi, A. C. (2016). Oral and maxillofacial pathology (4th ed., Ch. 3: Pulpal and Periapical Disease, Cellulitis and Ludwig Angina). Elsevier.
Cawson, R. A., & Odell, E. W. (2017). Cawson's essentials of oral pathology and oral medicine (8th ed., Ch. 31: Medical Emergencies). Elsevier.
Regezi, J. A., Sciubba, J. J., & Jordan, R. C. K. (2017). Oral pathology: clinical pathologic correlations (7th ed., Ch. 3: Pulpal and Periapical Disease). Elsevier.
Frequently asked questions
Is Ludwig's angina a medical emergency?
Yes. Ludwig's angina is a rapidly spreading bacterial infection of the floor of the mouth and neck that can swell the airway shut within hours. Anyone with significant swelling under the jaw, difficulty swallowing or any change in voice, breathing or drooling needs to be assessed urgently, often in a hospital emergency department.
What does Ludwig's angina look and feel like?
Typical features include a hard, board-like swelling under both sides of the jaw, a raised and stiff floor of the mouth, the tongue being pushed up and back, drooling, difficulty swallowing, muffled speech and fever. People often describe feeling unwell quickly over a day or two from what started as a sore tooth or sore throat.
What causes Ludwig's angina?
Most cases start from a dental infection, particularly an untreated lower molar abscess, that spreads downward into the soft-tissue spaces under the jaw and tongue. Other triggers include deep gum infections, jaw fractures, oral surgery or trauma. People with diabetes or weakened immunity are at higher risk.
How is Ludwig's angina treated?
Treatment is urgent and hospital-based. It typically involves protecting the airway, intravenous antibiotics, surgical drainage of the infected spaces, and addressing the dental source (such as removing the offending tooth) once the patient is stable. With prompt care the outlook is good; delayed treatment can be life-threatening.



