Compiled from clinical pathology references. Medically reviewed by Dr Cristian Dunker , Principal Dentist, ArtSmiles Cosmetic Dentistry.
Quick summary
Also called | Pulp death, non-vital (with a dead nerve) tooth, dead tooth, pulpal necrobiosis (when partial) |
How urgent? | 🟡 Worth a check-up, a tooth with a dead nerve usually needs treatment, even when it doesn't hurt, because infection can spread silently |
Common or rare? | Very common, one of the most frequent reasons for root canal therapy or tooth removal |
Who it affects | Both children and adults; very common in adults with deep decay or a history of dental trauma |
Who treats it | General dentist, sometimes with referral to an endodontist (root canal specialist, a dentist who specialises in this treatment) |
Based on | Regezi, Neville, Cawson |
What is it?
Pulp necrosis (death of the tissue) simply means the soft tissue inside your tooth has died. That soft tissue, called the pulp (the soft nerve and blood vessel core of the tooth), sits in a small chamber in the middle of the tooth and contains the nerve, blood vessels and connective tissue that keep the tooth alive and able to feel hot, cold and pressure. When the pulp dies, the tooth becomes what dentists call non-vital. The outer shell of enamel and dentine (the softer layer under the enamel) stays in place, but the living core inside no longer responds.
Who tends to get it?
Pulp necrosis can happen at any age and in any tooth, but a few patterns stand out in the literature.
It is most often seen in adults with longstanding deep decay or repeatedly restored teeth. Front teeth (the upper incisors in particular) are commonly affected after a knock to the face, sometimes a sporting injury or fall from years or even decades earlier. In children and teenagers, an injury to a still-developing front tooth can lead to pulp death before the root has finished forming. Molars become non-vital most often through deep cavities or large fillings.
There is no strong gender or ethnicity link, what drives risk is the history of the tooth itself, not the patient.
What causes it?
The pulp dies when its blood supply is cut off, when it is overwhelmed by infection, or both. The most common triggers described in the textbooks are:
Deep dental caries (decay), bacteria and their by-products travel through the dentine and inflame the pulp. If the inflammation becomes severe enough (irreversible pulpitis, inflammation of the pulp), the pulp eventually dies.
Trauma to the tooth, a blow to the face can damage the small vessels entering the root tip, choking off the blood supply. This can cause the pulp to die immediately, or quietly months to years later.
A cracked or fractured tooth, even a hairline crack can let bacteria in. Cracks under restored back teeth are a classic culprit and often hard to spot.
Deep or repeated fillings and crowns, heat, vibration or chemicals from dental procedures, especially when a filling is placed without an insulating base, can irritate the pulp. Each time a tooth is re-restored, the pulp takes another hit.
Severe gum disease (periodontitis), when bone loss reaches the root tip or a side canal, infection can travel up into the pulp.
Thermal or chemical irritation, large unlined metal restorations and some restorative materials can transmit heat or irritants over time.
These causes often stack on top of each other, for instance, a tooth with an old large filling that later cracks under chewing pressure.
How does it develop?
A helpful way to picture the pulp is as a finger of soft tissue squeezed inside a hard glove. There is only one small opening at the root tip for the blood vessels and nerve to enter and leave.
When the pulp becomes inflamed, usually from bacteria in a deep cavity, the tissue swells. But because the surrounding dentine cannot stretch, that swelling has nowhere to go. The pressure squashes the tiny blood vessels at the root tip, the blood supply is choked off, and the tissue inside slowly suffocates. This is sometimes called liquefaction necrosis when bacteria are the main driver, the pulp essentially digests itself into a soft, infected mass.
In trauma cases, the mechanism is different. A blow can shear or sever the vessels at the root tip directly, cutting off the blood supply in an instant. The pulp tissue then dies from lack of oxygen, a process called coagulation necrosis. The dead tissue often becomes secondarily infected by bacteria seeping in from the gum margin or through tiny cracks.
Whole pulp death is the usual end stage, but partial pulp necrosis (pulpal necrobiosis) is also recognised, for example, only one root canal of a multi-rooted molar may be affected while the others stay alive.
What might you notice?
What it looks like
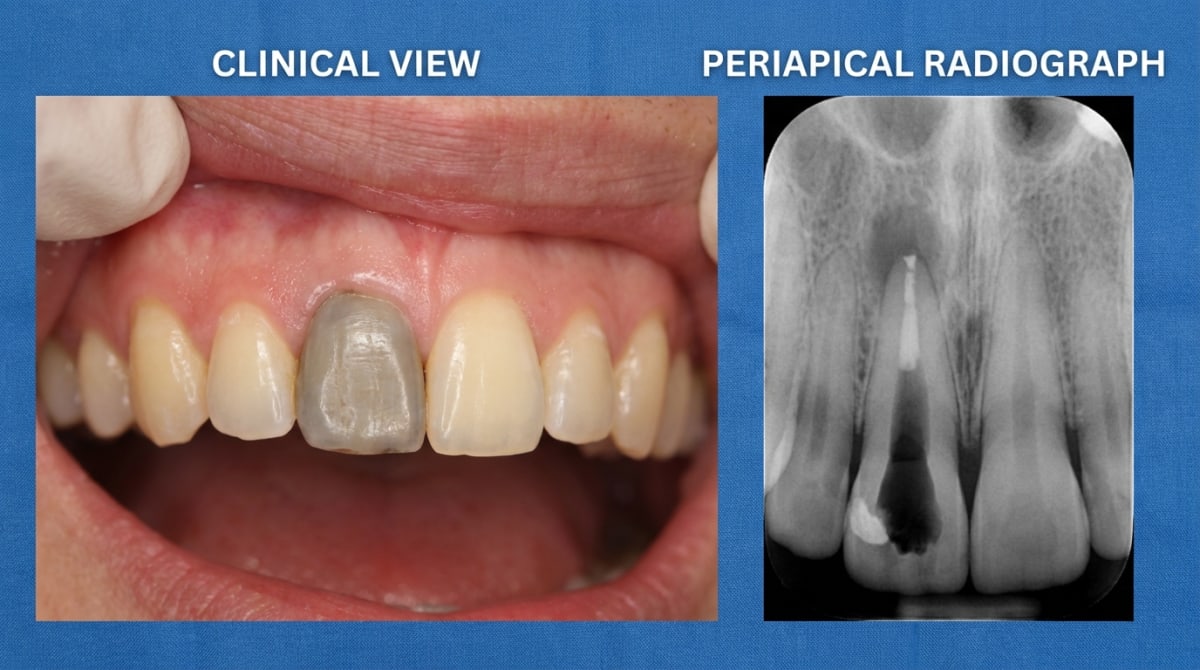
Many dead teeth look completely normal from the outside, especially in the early stages. Over time, however, a non-vital tooth, particularly a front tooth, may take on a darker shade than its neighbours. Classic colours described in the texts are grey, yellow-grey, brown or a dusky pink, caused by the breakdown products of blood and pulp tissue staining the dentine from the inside. This discolouration is a well-known late sign after dental trauma and may not appear for months or years after the original injury.
If the dead pulp becomes infected and the infection spreads beyond the root tip, you may notice a small pimple-like bump on the gum near the tooth (sometimes called a gum boil or sinus). It may release a salty or bad-tasting fluid when pressed.
What it feels like
This is where pulp necrosis can be deceiving. A tooth with a dead pulp is often completely painless. There are no living nerve endings left inside the tooth to send pain signals, so once the earlier inflammation has settled, the tooth can stay silent for months or even years.
When symptoms do occur, they tend to fall into a few patterns:
A history of severe, throbbing toothache (from the irreversible pulpitis stage) that mysteriously settled on its own, this often signals the pulp has died, not healed.
A dull ache or feeling that the tooth is "not quite right" when biting.
Tenderness on biting or tapping the tooth, which usually means infection has reached the tissues around the root tip.
An unpleasant taste or smell from the area, suggesting drainage of an infection.
Hot or cold no longer triggers any sensation, where it once did.
What an X-ray might show
In the early stages, a radiograph may look completely normal, the dead pulp itself is not visible. Over weeks to months, a slight widening of the dark line around the root tip (the periodontal ligament space) may appear. As infection progresses, a darker round patch develops at the root tip, this represents bone loss caused by chronic inflammation (a periapical granuloma, cyst or abscess). In some longstanding cases the pulp space inside the tooth may instead become narrower or partially filled in, particularly after trauma, a change called calcific metamorphosis (when the pulp slowly fills in with hard tissue).
What happens at the dentist?
Working out whether a pulp is alive or dead is one of the most important things a dentist does at ArtSmiles, because the answer shapes the whole treatment plan. Your dentist may:
Take a careful history, asking about past pain, knocks to the face (even years ago), large fillings, sensitivity changes and recent dental work.
Examine the tooth, checking for cracks, deep fillings, decay, swelling, gum tenderness and the colour of the crown compared to neighbouring teeth.
Tap the tooth gently (percussion test), a tooth that hurts when tapped often has inflammation around the root tip.
Test the pulp's response, usually with cold (a frozen cotton pellet or refrigerant spray) and sometimes with a small electric pulp tester. A tooth with a dead pulp typically gives no response to either. The texts note that pulp testing can occasionally be misleading, especially after trauma, so the dentist will usually combine several tests.
Take radiographs, to look for a widened space around the root tip, a darker patch of bone loss, root resorption, or signs of a crack.
Refer where appropriate, for tricky cases (multi-rooted teeth, teeth with very calcified canals, suspected cracks, or unclear test results), referral to an endodontist is sometimes recommended.
Is this serious?
🟡 Worth taking seriously, even when it doesn't hurt.
A non-vital tooth on its own is not a medical emergency. The danger is what tends to happen next. Once the pulp is dead, the inside of the tooth becomes a sheltered space that bacteria can quietly colonise, and the body has no way to fight infection there because there is no longer any blood supply. From the root tip, that infection can spread into the surrounding bone, forming a periapical abscess, granuloma or cyst. In rare but well-documented cases, infection from a dead tooth can spread further into the face, neck and beyond, with serious complications.
Untreated, the most likely path is gradual bone loss around the root, eventual loss of the tooth, and recurring flare-ups of pain and swelling along the way. The good news is that, when picked up early, pulp necrosis is very treatable.
If you've noticed any of these signs for more than two weeks, it's worth booking an assessment.
Could it be something else?
A tooth that aches, discolours or fails a vitality test can have several possible explanations. These are the most common look-alikes that a dentist will work through:
Reversible pulpitis, early, mild inflammation of a still-living pulp. Looks similar because the tooth is sensitive, but the tooth still responds normally (or briefly more intensely) to cold, and pain settles quickly when the trigger is removed.
Irreversible pulpitis, the stage just before pulp death. The pulp is still alive but inflamed beyond recovery; pain is severe, lingering and often spontaneous, and the tooth still responds to pulp testing (often dramatically). Pulp necrosis is the silent stage that follows.
Cracked tooth syndrome, a fine crack in a back tooth can mimic many of the same symptoms. Distinguished by sharp pain on biting that releases when pressure is removed, often only in one direction, and by transillumination or dye tests showing the crack.
Periodontal (gum) abscess, a localised gum infection that can also cause swelling and tenderness near a tooth. The tooth itself is usually still vital, and the problem traces back to a deep gum pocket rather than the pulp.
Calcific metamorphosis (pulp canal obliteration), after trauma, the pulp space slowly fills in with hard tissue. The tooth often appears yellow and gives a reduced or absent response to vitality testing, but periapical bone usually stays healthy. Many of these teeth never become infected and may not need treatment.
internal resorption ("pink tooth of Mummery", when the pulp gradually dissolves the inside of the tooth), abnormal cells eat away at the dentine from inside the pulp, sometimes giving the tooth a pink colour. Distinguished by a balloon-like widening of the canal on radiographs, in contrast to a normal-shaped canal in pulp necrosis.
Pulp calcifications (pulp stones), small mineralised bodies inside a still-vital pulp. Often picked up incidentally on radiographs and not usually painful; the pulp continues to test as alive.
Acute or chronic apical periodontitis, inflammation in the bone around the root tip. This is almost always a consequence of pulp necrosis rather than a separate condition, but can sometimes be the first sign noticed.
Sinusitis (referred upper-tooth pain), pain in upper back teeth from inflamed sinuses can mimic toothache, but the affected teeth still test as vital and pain shifts with head position or coincides with cold and nasal symptoms.
Periapical cyst, granuloma or abscess, these explain the dark patch on the X-ray that often comes with pulp necrosis, rather than being separate diagnoses.
How is it treated?
Once the pulp has truly died, it cannot be brought back. Treatment focuses on removing the dead tissue and any infection so the tooth can stay in the mouth without causing further problems.
At home (before and after treatment):
Keep up gentle but thorough brushing and flossing around the tooth.
Avoid biting hard on the affected side until you're seen.
Over-the-counter pain relief (such as ibuprofen, where suitable for you) can help in the meantime, but pain relief alone will not treat the underlying problem.
Don't ignore a tooth that has gone strangely quiet after a previous toothache, book in for a check.
Professional treatment may include:
Root canal therapy (endodontic treatment), the most common option for a tooth that is otherwise restorable. The dentist removes the dead pulp, cleans and disinfects the canal system, then fills and seals it. This is usually completed over one to three visits, and the tooth typically receives a strong final restoration (often a crown) afterwards to protect it from fracture.
Pulpotomy, in baby (deciduous) teeth, the inflamed or dying pulp in the crown of the tooth can sometimes be removed while leaving the deeper root pulp in place. This is a common approach in children to keep the baby tooth working until the adult tooth comes through.
Drainage of an abscess, if there's an active swelling or pus collection, the dentist will usually drain it (through the tooth or the gum) and may prescribe antibiotics if there are signs of spreading infection or systemic involvement. Antibiotics alone do not treat pulp necrosis, the source still needs to be dealt with.
Apical surgery (apicectomy), for cases where root canal therapy has not fully resolved the problem, a small surgical procedure may be recommended to clean the area around the root tip and seal it from below. This is more often used after retreatment of a root canal has been considered.
Extraction, if the tooth is too broken down, fractured below the gum, or otherwise non-restorable, removing it is sometimes the most predictable option. This is then followed by a discussion of replacement options.
Internal bleaching, for a discoloured front tooth that has had successful root canal therapy, bleaching from inside the tooth can often improve the appearance. Where the change is associated with a large restoration, full coverage (a crown or veneer) may be discussed.
Which path is right depends on how much sound tooth structure remains, the state of the surrounding bone, and your overall dental priorities, your dentist will talk this through with you.
What's the long-term outlook?
Pulp necrosis itself doesn't reverse, once the pulp has died, the tooth will need treatment to stay healthy long-term. The good news is that the prognosis for treated teeth is generally very favourable.
Well-completed root canal therapy followed by a sound final restoration has a high success rate, with most teeth remaining comfortable and functional for many years. The textbooks emphasise two key factors: the quality of the root canal treatment itself, and the quality of the restoration placed on top, even an excellent root canal can fail if the crown leaks. Follow-up radiographs at one and two years (and often sooner) are recommended to confirm the bone around the root tip is healing.
If treatment is delayed, the outlook is less predictable. A persistently infected dead tooth can cause progressive bone loss, recurring flare-ups, and eventually need extraction. Catching it early, before infection has spread or the tooth has fractured, gives the best chance of keeping the natural tooth in place for the long haul.
A note on this article
This article is for educational purposes only and does not constitute a clinical diagnosis. Please consult a registered dental practitioner for assessment and treatment advice.
The cover image above is an AI-generated illustration based on the most common visible features of this condition described in clinical pathology references. It is not a photograph of a real case and should not be used to diagnose or rule out the condition in your own situation. If you are concerned about something you have noticed, please book an assessment with a registered dental practitioner.
References
Regezi, J. A., Sciubba, J. J., & Jordan, R. C. K. (2017). Oral pathology: Clinical pathologic correlations (7th ed.). Elsevier. Chapter 13, Inflammatory Jaw Lesions: Pulpitis and Periapical Abscess, pp. 313 to 319.
Neville, B. W., Damm, D. D., Allen, C. M., & Chi, A. C. (2023). Oral and maxillofacial pathology (5th ed.). Elsevier. Chapter 3, Pulpal and Periapical Disease: Pulpal Necrosis, Periapical Granuloma and Cyst, pp. 117 to 128.
Cawson, R. A., & Odell, E. W. (2017). Cawson's essentials of oral pathology and oral medicine (8th ed.). Elsevier. Chapter 4, Pulpitis, Apical Periodontitis, Resorption and Hypercementosis, pp. 60 to 69.
Frequently asked questions
What does it mean if my tooth pulp has 'died'?
Pulp necrosis means the nerve and blood-supply tissue inside the tooth has died, usually from advanced decay, a deep crack or significant trauma. The tooth itself can still stay in the mouth, but it can no longer feel hot, cold or pressure normally. Without treatment, the dead tissue eventually becomes infected and produces an abscess.
Why is my tooth darker than the others?
A tooth with a necrotic pulp often gradually darkens to a grey, brown or yellow shade as breakdown products from the dead tissue stain the dentine from the inside. The change is most noticeable on front teeth and tends to develop slowly over months.
How is pulp necrosis treated?
Treatment is either root canal treatment (cleaning out the dead tissue and sealing the canals to save the tooth) or extraction if the tooth cannot be restored. Internal bleaching can sometimes lighten the darkened crown after root canal treatment, or a veneer or crown can mask the discolouration.
Can a tooth with a necrotic pulp heal on its own?
No. Once the pulp tissue has died, it does not regenerate. The body cannot remove the dead tissue from inside the tooth, so it remains a source of low-grade infection unless treated. Definitive treatment (root canal or extraction) is needed to resolve the problem.



