Compiled from clinical pathology references. Medically reviewed by Dr Cristian Dunker , Principal Dentist, ArtSmiles Cosmetic Dentistry.
Quick summary
Also called | Radiation-induced oral inflammation of the mouth lining (mucositis), radiotherapy mucositis, oral mucositis (when caused by head and neck radiotherapy) |
How urgent? | 🔴 See your dental and oncology team promptly, it is expected during treatment, but pain, dehydration and infection need active management |
Common or rare? | Very common, affects almost every patient receiving radiation therapy to the head and neck for deep tumours |
Who it affects | Adults receiving radiotherapy (with or without chemotherapy) for cancers of the mouth, throat, larynx, salivary glands or nearby structures |
Who treats it | A combined team, radiation oncologist, medical oncologist, dentist or oral medicine specialist, dietitian and specialist nurse |
Based on | Regezi, Neville, Cawson, Laskaris |
What is it?
Radiation mucositis is the painful inflammation and breakdown of the lining of the mouth and throat caused by radiation therapy to the head and neck. The mouth lining (mucosa) first turns red and sore, then loses its surface, and finally develops large ulcers covered by a yellowish-white film. It is the single most debilitating short-term complication of head and neck radiotherapy, and almost everyone who receives this treatment to a meaningful dose will experience it to some degree.
Who tends to get it?
Radiation mucositis is part of the package for patients receiving radiotherapy to the oral cavity, oropharynx (the back of the throat behind the soft palate), larynx (voice box), nasopharynx (the upper throat behind the nose) or salivary glands. Almost all patients receiving radiation therapy to the head and neck for deeply seated tumours will develop it. The risk is higher when radiotherapy is given together with chemotherapy (chemoradiation), which is now common practice for advanced disease.
A few features make it more severe or more difficult:
A radiation dose above 50 Gray (Gy, the unit doctors use for radiation amount) to the mucosa, with most courses for oral cancer being around 60 Gy or higher
Concurrent chemotherapy alongside radiotherapy
Poor oral hygiene or active dental infection at the start of treatment
Tobacco use and alcohol consumption during therapy
Poor nutrition or impaired salivary function before treatment begins
Younger age and female gender are associated with more severe mucositis in some studies
What causes it?
The direct cause is the radiation itself. Ionising radiation (high-energy radiation that damages cells in its path) is aimed at the tumour, but it cannot avoid the normal mucosa within the treatment field. The cells lining the mouth divide rapidly to keep the surface intact, and rapidly dividing cells are exactly the cells most sensitive to radiation damage.
Several factors influence how severe the mucositis becomes:
Total dose and how it is delivered. Higher cumulative doses and larger fractions cause more damage. Spreading the dose over many small daily fractions limits but does not prevent injury.
The size of the radiation field. A wider beam exposes more mucosa.
Concurrent chemotherapy. Drugs such as cisplatin and 5-fluorouracil add their own toxicity to the lining of the mouth.
Pre-existing oral health. Plaque, untreated decay, periodontal disease and ill-fitting dentures all worsen the local picture.
Lifestyle factors during treatment. Continued smoking and alcohol use prolong and intensify symptoms.
How does it develop?
Think of the lining of the mouth as a thin sheet of tissue paper that is constantly being replaced from underneath. Healthy basal cells (the deep layer) divide every few days to push fresh cells up to the surface, where they wear away with normal use. Radiation works partly by damaging the DNA of dividing cells, which is why it is good at killing cancer, but the basal cells of the mouth divide just as quickly as the tumour cells.
When the basal layer is damaged, the surface keeps wearing away as usual, but there is nothing coming up to replace it. Over a couple of weeks, the mucosa becomes thinner, then patchy, then frankly ulcerated. At the same time, radiation triggers the release of inflammatory signals (cytokines and reactive oxygen species) within the tissue, which amplifies the swelling, redness and pain.
This is why mucositis follows such a predictable timeline:
Week 1: redness (erythema) and swelling appear at the end of the first week, with a faint white look from retained surface keratin (the tough surface protein of the mouth lining)
Week 2 onwards: small erosions and ulcers begin to appear, often covered by a whitish-yellow exudate
Weeks 4 to 6: symptoms typically peak, with widespread (confluent) painful ulcer formation through the treatment field
2 to 6 weeks after the last session: the mucosa gradually heals as the basal layer recovers
What might you notice?
What it looks like
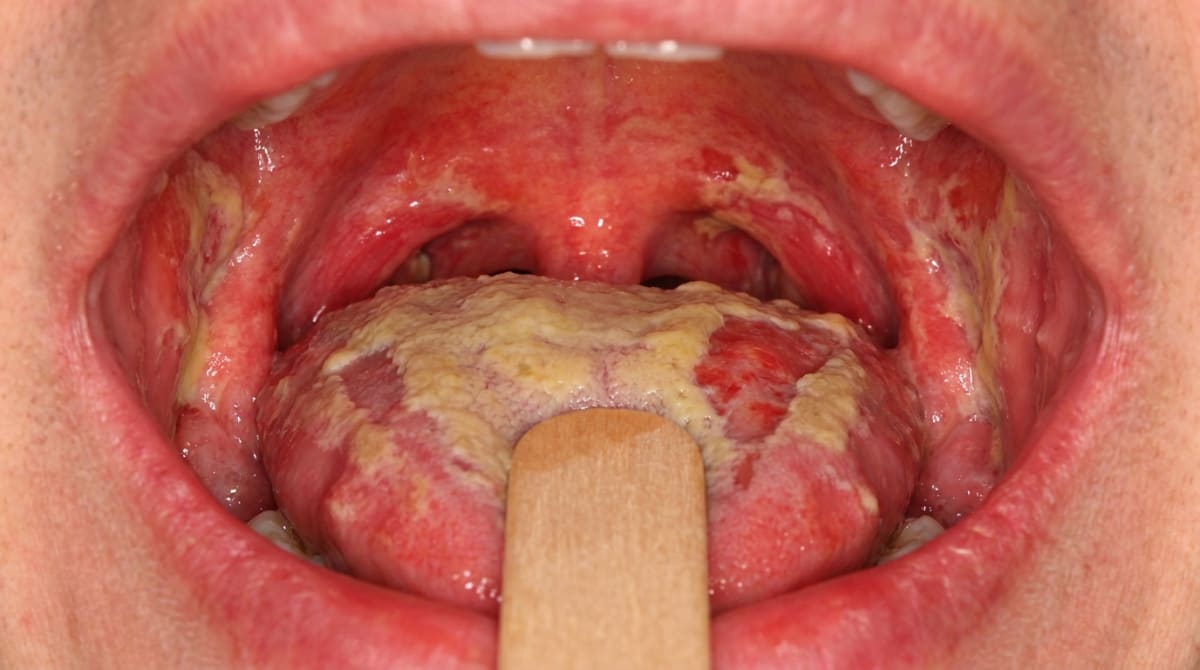
In the first week, the lining of the mouth and throat looks redder than usual and slightly swollen. By the second week, you may see small erosions where the surface has come away. As treatment continues, these merge into larger areas of ulceration, which are typically covered by a removable yellowish or whitish-yellow film (a fibrinopurulent membrane). The cheeks, soft palate, floor of the mouth and the underside and side of the tongue are most often affected, with the changes following the path of the radiation beam.
The lips, tongue and cheek can also look dry, shiny and atrophic (thinned), a direct consequence of damage to the salivary glands within the field.
What it feels like
The overwhelming symptom is pain. Patients commonly describe:
Burning or rawness across large parts of the mouth and throat
Sharp pain when eating, especially with anything spicy, acidic, salty or hot
A constant ache that worsens with brushing or rinsing
Difficulty swallowing (food, drinks and even saliva)
A persistent dry mouth, with thick or stringy saliva
Loss of taste, or food tasting metallic, bitter or simply absent
Speech becoming uncomfortable or muffled
Many patients lose weight during treatment because eating becomes too painful, and dehydration is a real risk. Fungal overgrowth (oral thrush) is common on top of the mucositis and can make the burning worse.
What an X-ray might show
Radiation mucositis itself is a soft-tissue change and is not seen on an X-ray. However, imaging is sometimes used during follow-up to look for the longer-term bony complication of head and neck radiotherapy, osteoradionecrosis (a long-term breakdown of irradiated jawbone), which can show as poorly defined areas of bone breakdown in the jaw, usually the mandible (the lower jaw).
What happens at the dentist?
Dental input ideally starts before radiotherapy begins, not after symptoms appear. A pre-treatment dental assessment is one of the most important things that can be done to reduce both the severity of mucositis and the risk of later complications such as osteoradionecrosis. At ArtSmiles, this is coordinated alongside your oncology team.
A typical pathway looks like this:
Before radiotherapy. Your dentist may carry out a thorough exam, take any necessary X-rays, complete a professional clean and remove plaque and tartar. Teeth that are unrestorable, severely decayed, or have advanced periodontal disease are usually extracted, ideally with at least three weeks of healing before radiation begins. Custom-fitted soft fluoride trays may be made for nightly fluoride application.
During radiotherapy. Examination focuses on grading the mucositis (using a recognised scale such as the WHO scale, which runs from 0 for normal to 4 for tissue requiring tube feeding), looking for secondary fungal or bacterial infection, and supporting pain control and nutrition.
After radiotherapy. Lifelong follow-up checks watch for radiation-related caries, persistent dry mouth, taste changes and any signs of osteoradionecrosis or recurrent or new cancer.
A biopsy is rarely needed for the mucositis itself, the diagnosis is based on the history of recent radiation and the clinical picture. A swab may be taken if a fungal or bacterial infection is suspected.
Is this serious?
🔴 Radiation mucositis is a serious but expected complication that needs active management throughout treatment.
Untreated or poorly controlled mucositis can:
Cause severe pain that requires opioid analgesia (strong morphine-style pain medications)
Lead to significant weight loss, dehydration and the need for a feeding tube (nasogastric or PEG tube)
Allow secondary candidiasis and bacterial infection, including, in immunosuppressed patients, bacteraemia and sepsis (bacteria entering the bloodstream and a body-wide reaction to infection)
Result in unplanned breaks in the radiation schedule, which may reduce the chance of cure
The good news is that the mucositis itself is reversible. The mucosa typically begins to heal within a couple of weeks of finishing radiotherapy and is largely settled by 4 to 6 weeks afterwards. Late effects such as dry mouth, taste change, scarring (fibrosis) and increased caries risk can, however, persist long term.
If you are receiving head and neck radiotherapy and your mouth pain, swallowing or weight is changing rapidly, contact your oncology team or dental team straight away.
Could it be something else?
In a patient who is partway through head and neck radiotherapy, the diagnosis is usually clear from the history. There are, however, several conditions that can look similar or develop on top of radiation mucositis:
Chemotherapy-induced mucositis, cancer drugs alone can cause similar painful ulceration, but the changes appear within a few days of treatment (rather than after a week or two), tend to favour the non-keratinised areas (cheeks, underside of tongue, soft palate, floor of mouth) rather than following a radiation field, and are not limited to the area being radiated.
Oral candidiasis (thrush), fungal overgrowth is common during radiotherapy and adds creamy-white removable plaques or smooth red sore areas on top of the mucositis. Smear or swab tests, and the response to antifungal medication, help to tell them apart.
Recurrent or residual cancer, a persistent ulcer that does not heal in the expected timeframe after radiotherapy, especially with raised or rolled edges, may need biopsy to exclude returning squamous cell carcinoma.
Herpes simplex virus reactivation, in patients on chemotherapy or who are otherwise immunosuppressed, herpes can produce painful clusters of small ulcers, often starting on the lips or hard palate. Viral swabs help confirm the cause.
Necrotising mucositis, severe gum or palatal tissue breakdown driven by bacteria such as Capnocytophaga and Fusobacterium, more often seen in profoundly immunosuppressed cancer patients. The pattern of necrosis, bacterial culture and response to antibiotics distinguish this from radiation injury alone.
Graft-versus-host disease (an immune reaction after a bone marrow transplant), in patients who have had a bone marrow transplant, lichen-planus-like white striae, ulcers and dry mouth can occur. The history of transplantation and the typical lacy appearance help identify it.
Allergic contact stomatitis, reactions to mouthwashes, flavourings or dental materials can cause redness and erosions, but they are usually localised to the area of contact rather than the whole radiation field.
Radiation dermatitis (skin), outside the mouth, redness, peeling and ulceration of the skin within the beam path are an expected parallel finding, and not a different diagnosis.
How is it treated?
There is no single drug that completely prevents radiation mucositis. Care is built around prevention before treatment, supportive measures during treatment, and active management of pain, infection and nutrition.
Before radiotherapy starts
A pre-treatment dental assessment, professional clean, and removal of unrestorable or infected teeth
Custom fluoride trays and fluoride toothpaste to protect against radiation-related caries for life
Smoking cessation and reduced alcohol use
Nutritional review with a dietitian
During radiotherapy, keeping the mouth as comfortable as possible
Frequent gentle rinses with bland salt-and-bicarbonate solutions, or plain saline
Avoiding alcohol-based mouthwashes, hot, spicy, acidic, crunchy or coarse foods
A soft, bland, high-protein and high-calorie diet, with thickened liquids if swallowing is painful
Regular gentle brushing with a soft toothbrush and a non-foaming toothpaste
Treatment of fungal overgrowth with antifungal lozenges, suspensions or systemic antifungals as prescribed
Treatment of secondary bacterial infection with antibiotics where indicated
Pain relief stepped up as needed, from simple analgesics through to topical anaesthetic rinses (sometimes called "magic mouthwash", a compounded mix typically containing a local anaesthetic, an antihistamine and a coating agent) and on to systemic opioids when pain is severe
Specific preventive options that may be considered
Low-level laser therapy (also called photobiomodulation, a low-power red-light treatment applied inside the mouth) has been shown to reduce the severity and duration of mucositis in selected patients receiving head and neck radiotherapy and is recommended in international supportive-care guidelines
Benzydamine mouthwash, a topical anti-inflammatory, may be recommended for patients receiving head and neck radiotherapy
Palifermin (a man-made version of keratinocyte growth factor, a natural protein that helps the mouth lining renew) is approved specifically for high-dose chemotherapy and total body irradiation before bone marrow (haematopoietic stem cell) transplantation, not for routine head and neck radiotherapy
Cryotherapy (sucking ice chips) helps with certain short-acting chemotherapy drugs but does not help radiation mucositis
Modern radiation techniques such as intensity-modulated radiation therapy (IMRT) and three-dimensional conformal radiotherapy (3DCRT) reduce the volume of normal mucosa irradiated and have lowered the severity of mucositis and the risk of osteoradionecrosis
When the mouth simply cannot keep up
If eating and drinking become impossible despite supportive care, your team may recommend short-term feeding through a nasogastric tube, or longer-term feeding through a PEG (a small tube placed through the abdominal wall into the stomach), so that nutrition and hydration are maintained until the mouth heals.
Treatment is always coordinated with the oncology team, and decisions are made in the context of the cancer being treated.
What's the long-term outlook?
The acute mucositis itself almost always resolves. The lining of the mouth begins to repair within a couple of weeks of the last radiation session, and most patients have largely settled, healed mucosa by 4 to 6 weeks after treatment ends.
Several consequences of head and neck radiotherapy can, however, last much longer:
Persistent dry mouth (xerostomia). Salivary tissue, especially the parotid glands (the large glands in front of the ears), is very sensitive to radiation. Some recovery is often seen at lower doses, but many patients are left with significantly reduced saliva. The mucous glands (the ones producing thick saliva) tend to recover better than the serous glands (the ones producing watery saliva).
Taste changes. Most taste recovers within around 4 months of finishing treatment, but some patients are left with reduced or altered taste long term.
Increased caries risk. Reduced saliva and changes within the teeth themselves lead to a particular pattern of cervical ("radiation") caries, which is why lifelong daily fluoride and regular dental review are so important.
Mucosal atrophy and telangiectasia. The lining can stay thin, shiny and easily damaged, with fine surface blood vessels visible.
Trismus (limited jaw opening) if the muscles of mastication or the temporomandibular joint were in the radiation field.
Osteoradionecrosis. The risk of bone breakdown, usually of the mandible, never fully goes away. It is highest in the first three years but persists for life, especially after dental extractions or trauma in irradiated bone.
With good pre-treatment dental preparation, careful supportive care during radiation, and ongoing dental review, most people get through radiation mucositis safely. Outcomes are generally better when patients have access to a coordinated team and start dental care before radiotherapy begins.
A note on this article
This article is for educational purposes only and does not constitute a clinical diagnosis. Please consult a registered dental practitioner for assessment and treatment advice.
The cover image above is an AI-generated illustration based on the most common visible features of this condition described in clinical pathology references. It is not a photograph of a real case and should not be used to diagnose or rule out the condition in your own situation. If you are concerned about something you have noticed, please book an assessment with a registered dental practitioner.
References
Regezi, J. A., Sciubba, J. J., & Jordan, R. C. K. (2017). Oral pathology: Clinical pathologic correlations (7th ed.). Elsevier. Chapter 2, Ulcerative Conditions (Therapeutic Radiation Complications), pp. 70 to 72.
Neville, B. W., Damm, D. D., Allen, C. M., & Chi, A. C. (2023). Oral and maxillofacial pathology (5th ed.). Elsevier. Chapter 8, Physical and Chemical Injuries (Oral Complications of Cancer Therapy: Mucositis, Xerostomia, Osteoradionecrosis), pp. 281 to 286.
Cawson, R. A., & Odell, E. W. (2017). Cawson's essentials of oral pathology and oral medicine (8th ed.). Elsevier. Chapter 17, Oral Cancer (Treatment and Unwanted Effects of Radiotherapy), pp. 286 to 287; Chapter 24, Immunodeficiencies and HIV Disease (Bone Marrow Transplantation Complications), p. 351.
Laskaris, G. (2003). Color atlas of oral diseases (3rd ed.). Thieme. Chapter 9, Radiation-induced Injuries, pp. 80 to 82.
Frequently asked questions
What is radiation mucositis?
Radiation mucositis is inflammation, redness and ulceration of the lining of the mouth caused by radiotherapy to the head and neck. It usually appears in the second week of treatment, peaks in weeks 4-6, and gradually heals over the 2-4 weeks after radiotherapy ends. It is one of the most uncomfortable side-effects of head-and-neck cancer treatment.
What does it look like?
Mucositis progresses from generalised redness (mild) to patchy white pseudomembrane (moderate) to confluent ulceration with bleeding (severe). Pain is significant, eating and swallowing become difficult, and weight loss is common. Long-term effects include persistent dryness (from salivary gland damage), increased decay risk and rarely osteoradionecrosis of the jaw.
How is radiation mucositis prevented or managed?
Prevention strategies include a pre-radiotherapy dental review (extracting unrestorable teeth, scaling, fluoride trays), meticulous oral hygiene, alcohol-free fluoride mouthrinses, salt-and-bicarbonate rinses, benzydamine mouthwash, low-level laser therapy and avoiding tobacco and alcohol. Photobiomodulation (low-level laser) is now recommended as preventive.
What treatments help during a flare?
Symptomatic relief includes topical anaesthetics (lidocaine, benzydamine, magic mouthwash), opioid analgesics for severe pain, antifungal treatment of secondary candida overgrowth, antibacterial mouthrinses, soft bland diet (protein shakes, smoothies, soft food) and feeding support (NG tube or PEG) if oral intake cannot be maintained. Continuing good oral hygiene throughout is crucial.



