Reviewed by Dr Cristian Dunker, BDSc.
This article is general educational information from the ArtSmiles Dental Library. It is not individual clinical advice and isn't a substitute for an in-person assessment.
Two distinct chemical processes can damage teeth: bacterial decay (caries) driven by sugar, and direct erosion driven by acid. They look different on examination, they have different prevention strategies, and they often happen at the same time in the same mouth. Understanding the difference, and the timing of how each works, makes the practical advice make sense.
This article covers what actually happens at the tooth surface during an acid attack, the difference between decay and erosion, why frequency dominates the damage calculation, and how saliva and fluoride repair small damage between exposures.
Table of Contents
What enamel is and what it can lose
Enamel (the hard outer layer of the tooth) is roughly 96% mineral, mainly hydroxyapatite, a calcium-phosphate crystal. The remaining 4% is water and trace organic material. It is the most mineralised tissue in the body and the most acid-resistant, but it is not infinitely tough. Below a certain pH (a measure of acidity, where lower numbers mean more acidic), the calcium and phosphate begin to dissolve out of the crystals. This loss is called demineralisation.
The threshold pH for enamel is about 5.5. Above that, the tooth is stable. Below it, mineral leaks out. The further below 5.5 the mouth pH drops, and the longer it stays there, the more mineral leaves. When enough mineral is lost, the surface breaks down and a cavity forms. Until then, the damage is potentially reversible.
The dentine (the softer layer of tooth tissue underneath the enamel) is more vulnerable. Its threshold pH is closer to 6.5. Once the gum has receded and the root surface is exposed, decay and erosion both move much faster.
How sugar causes decay
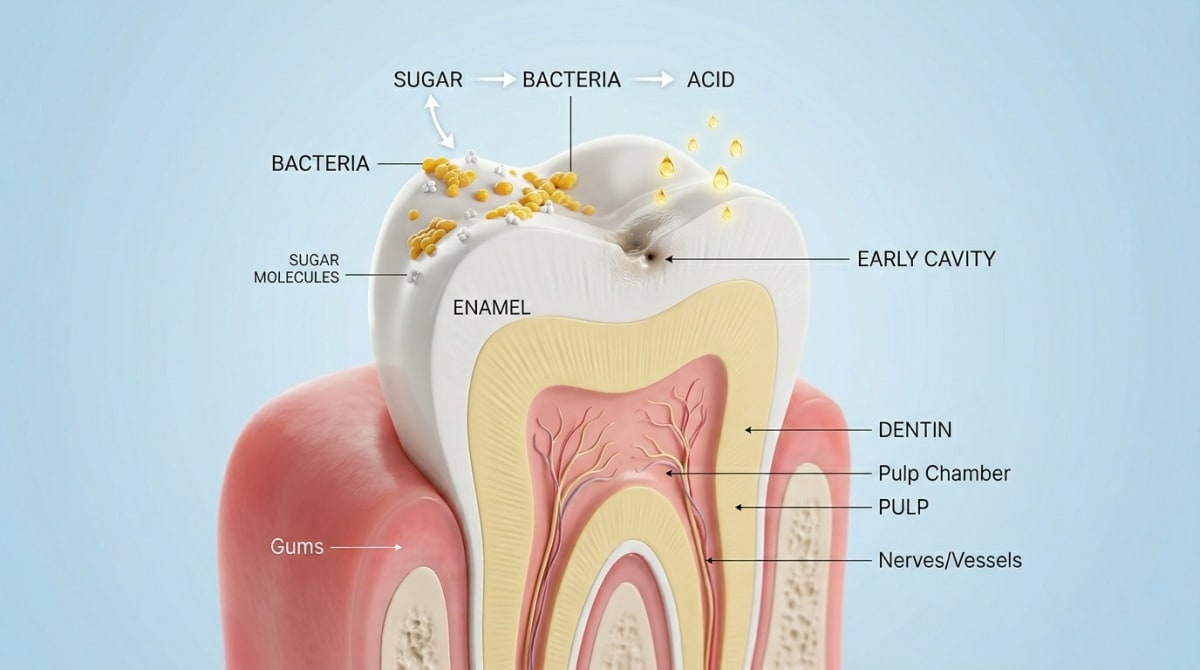
Sugar itself does not damage teeth directly. The damage is caused by the acid that bacteria produce when they ferment the sugar.
Specific bacterial species in dental plaque (the soft, sticky film of bacteria on the tooth surface) take in sugar from food and drink and metabolise it into lactic acid and similar organic acids. The pH at the tooth surface drops within a few minutes of sugar exposure, often to between 4 and 5, and stays there for about 20 to 40 minutes before saliva neutralises the acid and washes the residue away.
Each sugar exposure is a separate acid attack. A single chocolate biscuit eaten at the end of a meal causes one attack. A bag of lollies eaten one at a time across an afternoon causes ten or twenty. The total amount of sugar matters less than the number of separate exposures and how long each one lasts.
This is why sticky sugary foods (lollies, dried fruit, muesli bars) and slowly-sipped sweet drinks cause more damage per gram of sugar than the same amount eaten quickly with a meal. See Diet and Tooth Decay for the practical food-level guidance.
How acid causes erosion
Erosion is direct chemical damage from acid in food or drink, or from stomach acid, with no bacteria involved.
Common dietary causes include soft drinks (even sugar-free), fruit juices, sports drinks, wine, citrus fruits, vinegar dressings, kombucha, and apple cider vinegar. The acid lowers the mouth pH and dissolves the enamel surface directly. The pH of cola is around 2.5. The pH of lemon juice is around 2. These are well below the enamel threshold of 5.5, and the dissolution is rapid.
Internal sources of acid also matter. Frequent vomiting (from morning sickness, eating disorders, or chronic illness) bathes the back of the upper teeth in stomach acid. Gastro-oesophageal reflux disease (where stomach acid moves up into the oesophagus, sometimes reaching the mouth, often shortened to GORD or GERD) causes a similar pattern. The erosion in these cases tends to be on the inner (tongue-side) surfaces of the upper front teeth.
Erosion is often missed by patients because it does not cause pain in the early stages, and because the smooth shiny appearance of eroded enamel can look superficially clean. The signs are subtle thinning of the front teeth, increasing sensitivity to cold and acidic foods, and the gradual disappearance of the natural texture on the chewing surfaces.
Why frequency dominates the calculation
The single most useful concept in cavity prevention is the demineralisation-remineralisation balance.
After each acid attack, the teeth begin to recover. Saliva neutralises the acid, washes away food, and delivers calcium and phosphate that move back into the tooth surface. Fluoride from toothpaste, fluoridated water, and saliva itself accelerates the re-deposition. Over the next 20 to 60 minutes, the pH returns to neutral and the surface re-hardens.
If acid attacks are infrequent enough that the recovery time between them is longer than the attack, the balance favours re-mineralisation. The tooth stays stable.
If acid attacks are frequent enough that the recovery time is shorter than the attack, the balance favours demineralisation. The tooth gradually loses mineral, a white-spot lesion appears, and eventually a cavity forms.
This is why a single big sugary meal is often less damaging than a small constant trickle of sugar across the day. The total grams of sugar can be the same; the number and duration of acid attacks is very different.
How saliva and fluoride do the repair work
Saliva is the most underrated tooth-protecting fluid in the body. It buffers acid, washes the teeth, supplies calcium and phosphate, and contains antibacterial compounds. Anything that reduces saliva (medications, dehydration, mouth breathing, smoking, certain medical conditions) reduces the protective margin substantially. See Living with Dry Mouth for the patterns and the practical response.
Fluoride works in two main ways. It accelerates re-mineralisation, building the new mineral as fluorapatite, which is more acid-resistant than the original hydroxyapatite. It also reduces the acid output of plaque bacteria. Daily exposure through fluoride toothpaste is the simplest, most effective long-term protection. See Fluoride Explained for the dose ladder.
This is why "spit, do not rinse" after brushing matters. A small amount of fluoride toothpaste left on the teeth keeps re-mineralising over hours. Rinsing it off washes most of the protection down the sink.
What actual damage looks like
A few patterns are worth recognising.
Early decay (a white-spot lesion) appears as a chalky, dull patch on the smooth surface of a tooth or just below the gumline. The enamel is demineralised but the surface has not yet broken down. With improved cleaning, fluoride, and reduced sugar frequency, many of these lesions stabilise or reverse.
Established decay (a cavity) is a visible hole or a soft, sticky area on the tooth. The surface has broken down. The damage is permanent and a filling is the standard treatment.
Erosion appears as smooth, shiny, slightly cupped or scooped tooth surfaces, particularly on the chewing surfaces of the back teeth and the inner surfaces of the upper front teeth. Old fillings sometimes appear "raised" because the surrounding enamel has dissolved away.
Sensitivity to cold and to sweet is often the first patient-noticed symptom of any of these processes.
Practical implications
A few things follow logically from the chemistry.
Concentrate sugars at meal times. Three meals with sweets at the end produce three attacks. Sipping the same total sugar across the day produces many more.
Drink water as the default between meals. Water is pH neutral, washes the teeth, and supports saliva.
Rinse with water after acidic food or drink. Bring the pH back up before brushing.
Wait at least 30 minutes after acidic exposure before brushing. Brushing softened enamel scrubs the surface away.
Use a fluoride toothpaste twice daily, spit do not rinse. The single most useful protective habit.
Protect saliva. Avoid alcohol-based mouthwashes if your mouth is dry, manage medications that reduce saliva with your GP, and keep hydrated.
Treat reflux and frequent vomiting medically. Continuing to brush harder will not compensate for daily acid exposure from stomach acid.
Bottom line
Sugar causes decay through bacterial fermentation that produces acid for 20 to 40 minutes per exposure. Acid causes erosion directly without bacteria. Both processes are reversible at the early demineralised stage, given enough recovery time, saliva flow, and fluoride exposure. The single most useful protective principle is to limit the frequency of acid attacks (concentrate sugars at meal times, water as the between-meals default), rinse after acidic exposures, wait before brushing, and keep up the daily fluoride.
If you have noticed sensitive teeth, smooth shiny tooth surfaces, or new cavities at recent visits, our team at ArtSmiles can examine for the specific pattern, discuss the dietary contributors, and put together a prevention plan that fits.
Frequently asked questions
What is the difference between decay and erosion?
Decay is acid produced by bacteria fermenting sugars and refined carbohydrates. Erosion is direct chemical dissolution by dietary or stomach acid, with no bacteria involved. They look different on examination and require different prevention strategies.
How long does an acid attack last?
About 20 to 40 minutes for a single sugar exposure, longer if the food is sticky or sipped over time. Saliva needs at least 30 minutes to neutralise the acid and start re-mineralising the enamel.
Is honey better than sugar for teeth?
No. Bacteria ferment honey and sugar identically. The marketing distinction between "natural" and "refined" sugars is not relevant to dental decay.
Why does fizzy water damage enamel?
Carbonated water is mildly acidic (pH around 4 to 5) because of dissolved carbon dioxide. Plain carbonated water occasionally is not a major concern. Flavoured carbonated drinks add citric acid and become much more erosive.
Can early decay be reversed?
Early enamel demineralisation can re-mineralise if the cause is removed and fluoride is available. Once a cavity has formed (the surface has broken down), the tissue is not regenerated and a filling is needed.
Does brushing immediately after acid help or hurt?
It hurts. Brushing on softened enamel scrubs away the surface layer. Wait at least 30 minutes after acidic foods or drinks before brushing, or rinse with water and brush later.
References
Featherstone, J. D. B. (2008). Dental caries: A dynamic disease process. Australian Dental Journal, 53(3), 286 to 291.
Lussi, A., & Carvalho, T. S. (2014). Erosive tooth wear: A multifactorial condition of growing concern and increasing knowledge. Monographs in Oral Science, 25, 1 to 15.
Moynihan, P. J., & Kelly, S. A. M. (2014). Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. Journal of Dental Research, 93(1), 8 to 18.