Compiled from clinical pathology references. Medically reviewed by Dr Cristian Dunker, Principal Dentist at ArtSmiles Cosmetic Dentistry.
Quick summary
Also called | Residual periapical cyst, residual radicular cyst |
How urgent? | 🟡 Worth checking, usually painless but should be confirmed and treated to rule out other lesions and prevent slow jaw expansion |
Common or rare? | Common, one of the most frequently encountered cysts in the edentulous (no-teeth) jaw of older adults |
Who it affects | Adults, particularly older adults who have had teeth extracted years ago and now wear dentures or are edentulous |
Who treats it | General dentist, often in coordination with an oral and maxillofacial surgeon for the removal |
Based on | Cawson, Neville, Regezi |
What is it?
A residual cyst is a dental cyst that has been left behind in the jawbone after the responsible tooth has been removed. Most commonly it begins life as a radicular cyst, also called a periapical cyst, which forms at the tip of the root of a non-vital (dead-pulp) tooth. When the tooth is extracted but the cyst lining is not completely curetted out at the same time, the lining can persist and continue to enlarge slowly in the jaw. Sometimes the cyst was never noticed at the time of extraction and only becomes apparent years later. By definition, then, a residual cyst sits in an area where a tooth used to be, and it shares the same epithelial lining and pathology as the original radicular cyst.
Who tends to get it?
The textbooks describe residual cysts particularly in:
Older adults who have lost teeth, often years or decades earlier.
People in edentulous areas of the jaw, that is, areas where teeth are no longer present, including under partial or full dentures.
Patients who have had a tooth extracted because of long-standing decay or a deep filling, where a periapical cyst was already present at the time but was not enucleated.
Both jaws, although they are slightly more common in the mandible (lower jaw).
There is no strong sex predilection. Children are very rarely affected because the underlying radicular cyst takes time to develop in the first place.
What causes it?
A residual cyst develops in two stages:
Stage 1, formation of a periapical cyst. A tooth's pulp dies, usually from deep decay, a deep filling, repeated trauma, or a large crack. The dead tissue at the root tip drives chronic inflammation in the surrounding bone, forming first a periapical granuloma and, in many cases, eventually a periapical (radicular) cyst, lined by epithelium derived from microscopic remnants of the tissue that originally formed the tooth (rests of Malassez).
Stage 2, persistence after extraction. When the tooth is removed, the cyst lining can stay behind in the bone if it is not curetted out. The lining continues to produce fluid, and the cyst slowly enlarges into the residual cyst the X-ray finally reveals.
In some cases the original cyst may have been very small and unrecognised at the time of extraction. In others it may have been clearly visible but not removed because the focus was on extracting the tooth.
How does it develop?
Once the lining is established in the bone, the cyst grows in essentially the same way as a periapical cyst. The lining cells slough into the lumen, raising the protein content inside the cyst. Fluid is drawn in from the surrounding tissue to balance the osmotic pressure, and the cyst slowly enlarges. The bony wall around it is gradually resorbed, but at the same time the periosteum (the thin membrane covering the bone) lays down a thin shell of new bone over the surface. This is why a long-standing residual cyst can occasionally produce a thin "egg-shell" of bone that crackles when pressed during examination.
Most residual cysts grow slowly. Some appear stable for years, and Cawson notes that residual cysts may even slowly regress spontaneously as inflammation subsides, supported microscopically by progressive thinning of the cyst lining over time.
What might you notice?
What it looks like
Most residual cysts produce no visible change at all and are picked up on routine X-ray. When they do produce a change, it is usually:
A small bulge in the jawbone in an area where teeth are no longer present.
An area of swelling that the patient notices as a slight asymmetry in the jaw.
A denture that no longer fits as well as it used to, because the cyst is gradually expanding the bony ridge underneath.
Rarely, an eggshell-thin patch of bone that can crackle when gently palpated.
What it feels like
Most residual cysts are completely painless. When discomfort does occur, it is generally mild and may include:
A dull pressure under a denture as the cyst enlarges.
Soreness or ulceration if the overlying gum has become thinned.
A noticeable swelling that develops slowly over months or years.
Acute pain or rapid swelling only if the cyst becomes secondarily infected.
What an X-ray might show
The diagnosis is usually made on a panoramic dental X-ray or a periapical film. Typical findings:
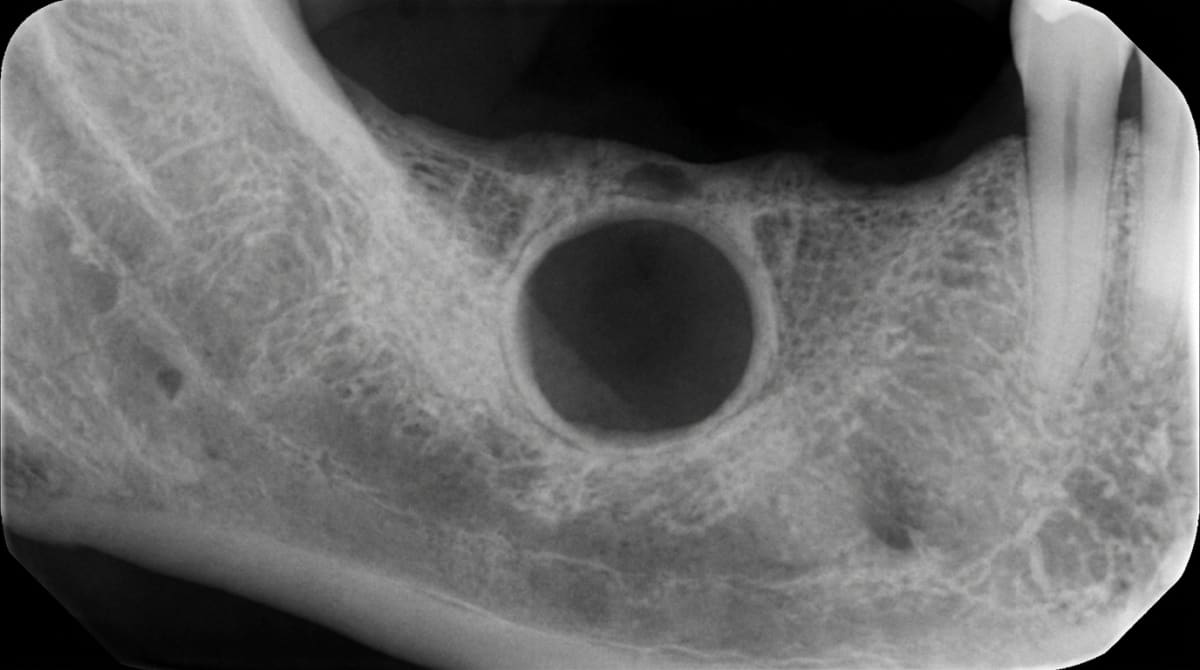
A well-defined, rounded or oval, dark (radiolucent) area within the alveolar ridge of an edentulous region.
A thin, well-corticated bony border outlining the cyst.
No tooth associated with the lesion, since the original tooth has long been extracted.
In some long-standing cysts, central calcifications may appear from old contents within the lumen.
A small-volume cone-beam CT (CBCT) scan is often the most useful tool for confirming size and exact relation to nerves, sinuses or adjacent teeth before any planned surgery.
What happens at the dentist?
A residual cyst is most often picked up at a dental check-up and clean at ArtSmiles when a routine panoramic X-ray is taken, for example, before starting denture work, considering implants, or planning other treatment. The dentist will typically:
Take a careful history about the history of extractions in that area, including how long ago, the reason for the extraction, and any past denture issues.
Examine the area for swelling, eggshell crackling, mobility of any neighbouring teeth, and changes in denture fit.
Take additional X-rays, periapical, panoramic, or a small-volume CBCT, to map the size and shape of the lesion.
Test the vitality of any neighbouring teeth to rule out an unrelated periapical lesion.
Aspirate the cyst in selected cases (drawing a small sample of fluid through a needle) to confirm it is fluid-filled.
Discuss whether the lesion needs surgical removal or whether ongoing review is appropriate, depending on size, growth pattern and overall health.
Refer to an oral and maxillofacial surgeon when the cyst is large or close to important structures such as the inferior dental nerve or the floor of the maxillary sinus.
Is this serious?
🟡 A residual cyst is benign, it is not cancer and does not spread. However, it is usually progressive and can cause:
Slow expansion of the jawbone.
Interference with denture fit or implant planning.
Erosion of the jawbone close to important structures such as the maxillary sinus or the inferior dental nerve.
Acute pain and swelling if it becomes infected.
For these reasons, most residual cysts are confirmed and removed once they are identified, even when they are not currently causing symptoms.
Could it be something else?
Several other conditions can produce a similar X-ray appearance in an edentulous area. The textbooks list these as the main differentials:
Surgical defect (healing socket), a recent extraction site can show as a radiolucency for many months while the bone fills in. The history clarifies this.
Anatomical structures, the maxillary antrum, the mental foramen, the incisive canal and the submandibular gland fossa can all be confused with a cyst on an X-ray. Position helps distinguish.
Ameloblastoma, a slowly growing benign tumour of the jaw that can mimic a cyst on a 2D X-ray. Usually multilocular and tends to expand the bone more aggressively.
Odontogenic keratocyst (OKC), another epithelial-lined cyst with a higher recurrence rate. Also can appear in edentulous areas.
Periapical granuloma at the retained root tip, if a small fragment of root was left in place at the time of extraction, ongoing inflammation can produce a radiolucency that resembles a residual cyst.
Primordial cyst, a less common cyst that develops in place of a tooth that never formed.
A definitive diagnosis usually requires histological examination of the tissue removed at surgery.
How is it treated?
Treatment is essentially surgical. Because the lesion is benign, the goal is to remove the entire cyst lining and confirm the diagnosis under the microscope.
At-home measures and habits:
Maintain excellent oral hygiene, including denture hygiene if you wear a denture, to reduce the risk of secondary infection.
Attend regular dental check-ups, including periodic X-rays where appropriate, so any change in size can be noticed and acted on early.
Report any changes in denture fit, mild swelling or new discomfort, since these may signal that the cyst is enlarging.
Professional steps your dentist may consider:
Surgical enucleation, the standard treatment, in which the entire cyst is gently shelled out of the bone in one piece. Cawson highlights enucleation as straightforward, with the cavity usually healing without complications.
Marsupialisation, for very large cysts close to important structures, the cyst may first be opened to the mouth and allowed to shrink before a definitive enucleation. This reduces the size of the eventual surgical defect.
Histopathological examination of the removed tissue is essential to confirm the diagnosis and rule out any rare unexpected diagnosis.
Bone grafting if a large defect remains after removal, particularly if the area is being prepared for a future implant.
Follow-up X-rays at intervals of 1 and 2 years to confirm complete healing and rule out recurrence.
Review of dentures or implants after healing, since the bone shape will have changed and existing dentures may need relining or replacing.
A patient-centred approach matters at every step, particularly for older patients who may be apprehensive about an additional procedure. Honest discussion about why the lesion needs to be addressed, what the surgery involves, and what to expect during healing is itself part of effective care, values that sit at the heart of our clinical philosophy.
What's the long-term outlook?
The outlook for a properly treated residual cyst is excellent. Once the cyst lining is fully removed, the bone usually heals over months and the lesion does not return. Recurrence after careful enucleation is uncommon. Where the cyst was particularly large, the bone may take longer to refill the defect, but most patients return to a fully functional jaw without long-term issues. Importantly, the original cause, a tooth that died and was not treated in time, is no longer present, so a "fresh" residual cyst will not arise from the same site. With ongoing dental care and regular X-rays, residual cysts are usually a one-off problem that is resolved and stays resolved.
A note on this article
This article is for educational purposes only and does not constitute a clinical diagnosis. Please consult a registered dental practitioner for assessment and treatment advice.
The cover image above is an AI-generated illustration based on the most common visible features of this condition described in clinical pathology references. It is not a photograph of a real case and should not be used to diagnose or rule out the condition in your own situation. If you are concerned about something you have noticed, please book an assessment with a registered dental practitioner.
References
Cawson, R. A., & Odell, E. W. (2017). Cawson's essentials of oral pathology and oral medicine (8th ed.). Elsevier. Chapter 7, Cysts of the Jaws: Residual cysts as persistent radicular cysts after extraction, denture interference, and possible spontaneous regression, pp. 119-120.
Neville, B. W., Damm, D. D., Allen, C. M., & Chi, A. C. (2023). Oral and maxillofacial pathology (5th ed.). Elsevier. Chapter 3, Pulpal and Periapical Disease: Residual Periapical Cyst with imaging and treatment guidance, pp. 127-129.
Regezi, J. A., Sciubba, J. J., & Jordan, R. C. K. (2017). Oral pathology: Clinical pathologic correlations (7th ed.). Elsevier. Chapter 10, Cysts of the Jaws and Neck: Residual cyst as a result of incomplete removal of cyst lining at extraction, pp. 247-248.
Frequently asked questions
What is a residual cyst?
A residual cyst is a jaw cyst that develops at, or was left behind from, the site of a previously extracted tooth. It originates from an inflammatory cyst (usually a radicular or periapical cyst) attached to the root of an infected tooth that was removed without the cyst lining being fully cleared at the time.
How is a residual cyst found?
Most are picked up by chance on a routine dental X-ray, often a panoramic image. The classic appearance is a well-defined dark area in the bone at the site of a previously extracted tooth, sometimes years after the extraction. They are usually painless unless they become infected.
Is a residual cyst dangerous?
It is benign and not cancer. Left alone, it tends to enlarge slowly and can thin the jawbone or press on neighbouring tooth roots and the inferior alveolar nerve. Surgical removal is recommended both to confirm the diagnosis and to prevent further enlargement.
How is a residual cyst treated?
Treatment is surgical excision (enucleation) under local anaesthetic. The cyst is lifted out of the bone and the wound is closed; the removed tissue is sent for microscopic examination. Recurrence is uncommon when the cyst is fully removed.



