Compiled from clinical pathology references. Medically reviewed by Dr Cristian Dunker , Principal Dentist, ArtSmiles Cosmetic Dentistry.
Quick summary
Also called | Follicular cyst |
How urgent? | 🟡 Worth checking, usually painless but progressive; can displace adjacent teeth, cause jaw expansion, and rarely lead to bone resorption if left for many years |
Common or rare? | The most common developmental cyst of the jaws, making up about 20% of all epithelium-lined jaw cysts |
Who it affects | Most often people aged 10-30, with a slight male predilection; almost always associated with an unerupted tooth, most commonly a lower wisdom tooth |
Who treats it | General dentist in coordination with an oral and maxillofacial surgeon; treatment is surgical |
Based on | Cawson, Neville, with cross-references in Regezi |
What is it?
A dentigerous cyst is a benign, fluid-filled sac that forms around the crown of an unerupted tooth. The cyst lining attaches to the tooth at the cementoenamel junction, the line where the enamel of the crown meets the cementum of the root, and the crown itself sits inside the cyst cavity. The textbooks describe it as developing through accumulation of fluid between the reduced enamel epithelium (the thin layer that originally covered the developing crown) and the enamel surface itself. Most dentigerous cysts are completely silent, picked up only when a dental X-ray is taken for another reason or to investigate a tooth that has not erupted. They are benign, but their slow expansion in the jaw means they generally need to be removed.
Who tends to get it?
The textbooks describe a relatively consistent profile:
Most often diagnosed between 10 and 30 years of age. They can occur at any age, but the peak is in adolescence and early adulthood.
Slightly more common in males than females.
Usually a single cyst affecting one unerupted tooth. Multiple dentigerous cysts are uncommon and may suggest a syndrome.
Around 65% involve mandibular third molars (lower wisdom teeth). Other common sites include maxillary canines (upper "eye teeth"), maxillary third molars (upper wisdom teeth) and mandibular second premolars.
Rarely involve baby (deciduous) teeth. Dentigerous cysts of baby teeth are unusual.
Very rarely associated with supernumerary (extra) teeth or with odontomas (developmental tooth-shaped masses).
What causes it?
A dentigerous cyst develops because fluid accumulates between the developing tooth and the soft tissue around its crown. The textbooks describe two main pathways:
Developmental origin (most common). As an unerupted tooth completes its enamel formation, a thin epithelial layer remains around the crown, called the reduced enamel epithelium. Fluid gradually accumulates between this layer and the crown, and the cyst forms.
Inflammatory origin (less common). In some cases, particularly in children, the dentigerous cyst around an unerupted permanent tooth seems to develop because of inflammation from an overlying baby tooth that has died. This can drive the lining of the dental follicle to form a true cyst.
The exact reason that some unerupted teeth develop a dentigerous cyst while others do not remains unclear. The textbooks note that the teeth most prone to dentigerous cyst formation, third molars and canines, are also the teeth most likely to fail to erupt, suggesting a connection between failure of eruption and cyst formation.
How does it develop?
Once a dentigerous cyst has formed, it tends to enlarge slowly. Fluid is drawn into the lumen by osmotic pressure, and the surrounding bone is gradually resorbed to make room. Three radiographic patterns of cyst-to-crown relationship are described:
Central variety (most common). The cyst surrounds the crown of the tooth, with the crown projecting into the cyst cavity.
Lateral variety. The cyst grows along the side of the root of a partially erupted, mesioangular (angled-forward) impacted lower wisdom tooth.
Circumferential variety. The cyst surrounds the crown and extends down the root for some distance, so that a significant portion of the root appears to lie within the cyst.
Over years, large dentigerous cysts can:
Displace the unerupted tooth a considerable distance, for example, a wisdom tooth pushed all the way to the lower border of the jawbone, or an upper canine pushed up toward the floor of the nose or even the floor of the eye socket.
Resorb the roots of adjacent erupted teeth.
Cause noticeable jaw swelling and, occasionally, facial asymmetry.
What might you notice?
What it looks like
Most dentigerous cysts produce no visible change. When they do, they may appear as:
A slow, painless swelling of the jawbone in the affected area.
A bulge under the gum near an unerupted tooth.
Facial asymmetry in long-standing, large cysts.
Occasionally, a bluish, soft swelling if the cyst is close to the mucosal surface (especially near an erupting tooth).
What it feels like
Uncomplicated dentigerous cysts are usually painless. Symptoms typically only develop when:
The cyst becomes infected (often from a partially erupted associated tooth, or from spread from an adjacent diseased tooth), pain, swelling, and sometimes pus.
The cyst becomes large enough to expand the jaw, producing a feeling of fullness, tightness or change in denture or appliance fit.
An adjacent tooth becomes mobile because of bone loss or root resorption (gradual loss of root structure caused by pressure or inflammation).
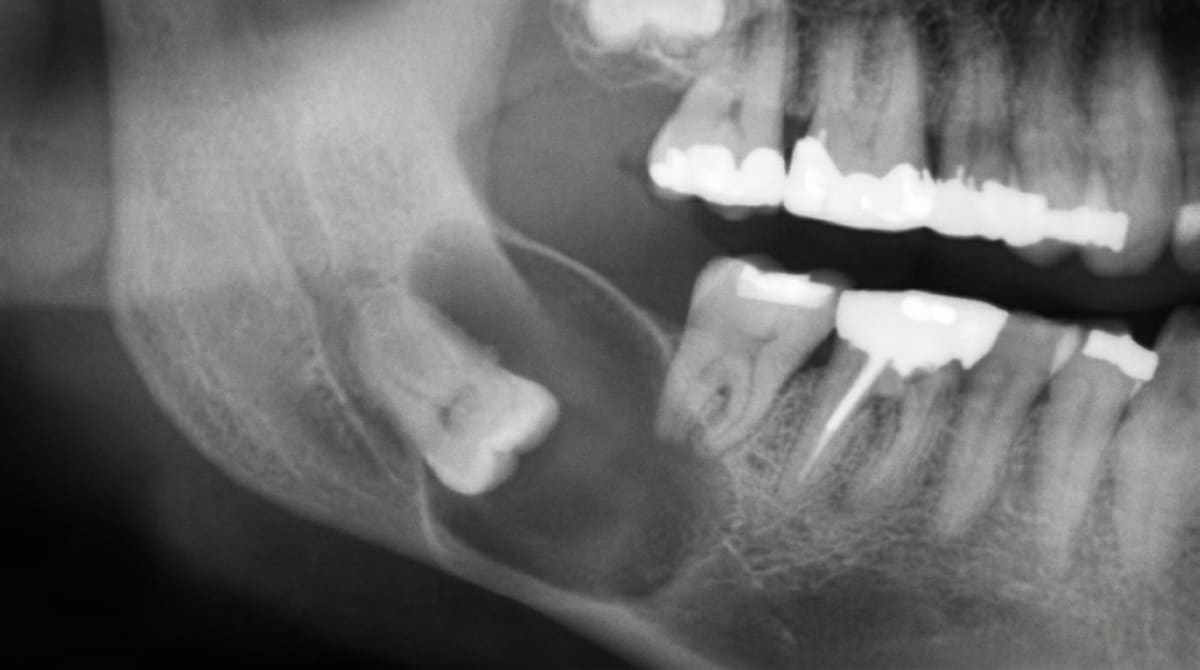
What an X-ray might show
Dentigerous cysts are usually picked up on a routine bite-wing or panoramic X-ray. Typical findings:
A well-circumscribed, unilocular (made of a single compartment, as opposed to multilocular which has multiple) (single-chamber), dark (radiolucent), darker on X-ray, indicating soft tissue or fluid rather than bone area surrounding the crown of an unerupted tooth.
A well-defined, often corticated (white) border outlining the cyst.
The cyst lining attached at the cementoenamel junction of the involved tooth.
Displacement of the unerupted tooth and sometimes the roots of nearby teeth.
Root resorption of nearby erupted teeth in long-standing cases.
Sclerotic bony outline because of the slow growth.
Sometimes a multilocular appearance, but this can be misleading and is usually due to bony ridging within a single cavity rather than true multiple chambers.
The textbooks specifically caution that radiographic features alone are not diagnostic, odontogenic keratocysts, unilocular ameloblastomas (benigns but locally aggressive tumour that can develop from cyst lining) and other lesions can look very similar. Final diagnosis requires histopathological examination after surgical removal.
What happens at the dentist?
A dentigerous cyst is typically picked up at a routine dental check-up and clean at ArtSmiles, often on a panoramic X-ray taken to assess wisdom teeth, plan orthodontic treatment, or investigate why a tooth has not erupted. The dentist will typically:
Take a careful history about how long the affected tooth has been missing or impacted, any past trauma, and any previous infections in the area.
Examine the mouth for swelling, mobility of adjacent teeth, gum bulging, and any partially erupted tooth nearby.
Take additional X-rays, periapical, panoramic, and often a small-volume cone-beam CT (a 3D dental X-ray, often shortened to CBCT) (CBCT) scan to map the cyst in three dimensions and check its relation to the inferior dental nerve, sinus, or other anatomical structures.
Test the vitality of adjacent teeth to rule out an inflammatory cause.
Discuss management options based on the size of the cyst, the importance of the involved tooth (an upper canine in a young patient is treated very differently from a wisdom tooth), and any risks to nearby structures.
Refer to an oral and maxillofacial surgeon when surgery is needed.
Is this serious?
🟡 A dentigerous cyst is benign and not cancerous. However, it generally needs to be addressed because it tends to enlarge, can displace teeth, can resorb adjacent roots, and may eventually thin or weaken the jawbone if left for many years. There are also rare reports of long-standing dentigerous cysts giving rise to ameloblastoma, mucoepidermoid carcinoma or squamous cell carcinoma in the cyst lining, although this is uncommon. For all of these reasons, dentigerous cysts are usually removed once they are identified.
If a routine X-ray has shown a fluid-filled sac around an unerupted tooth, it is worth booking an assessment so the size and position can be properly mapped and the right next step planned.
Could it be something else?
Several conditions can mimic a dentigerous cyst on an X-ray. The textbooks list these as the main differentials:
Odontogenic keratocyst (OKC), can also envelop the crown of an unerupted tooth and look identical on a 2D radiograph. Typically grows along the bone rather than expanding it. Has a higher recurrence rate than a dentigerous cyst, so accurate diagnosis matters.
Unilocular ameloblastoma, a benign but locally aggressive tumour that can also surround the crown of an impacted tooth. Can only be reliably distinguished by histopathology (examination of the removed tissue under the microscope).
Hyperplastic dental follicle, a normal but enlarged dental follicle around the crown of an unerupted tooth. Many investigators set a 3-4 mm radiolucent space around the crown as the threshold for calling a lesion a dentigerous cyst rather than just an enlarged follicle.
Eruption cyst, a soft tissue version of the dentigerous cyst that develops over a tooth that is about to erupt through the gum. Visible as a bluish swelling rather than as a bony lesion.
Lateral radicular cyst, at the side of an erupted, non-vital tooth. Less commonly confused but possible when the position is unusual.
How is it treated?
Treatment depends on the size of the cyst, the importance of the unerupted tooth, the age of the patient, and the relation of the cyst to nearby structures. The textbooks describe a clear range of options:
At-home measures and habits:
Maintain excellent oral hygiene to keep any partially erupted associated tooth as clean as possible and limit the risk of infection.
Attend regular check-ups and X-rays while a known dentigerous cyst is being monitored.
Report any new symptoms, swelling, pain, mobility, promptly, since these may signal infection or rapid enlargement.
Professional steps your dentist may consider:
Enucleation with extraction of the involved tooth, the standard treatment for dentigerous cysts associated with non-functional teeth such as impacted wisdom teeth. The cyst is shelled out together with its contained tooth in one piece, and the bone usually heals well.
Marsupialisation, in younger patients, where the cyst surrounds an important tooth such as an upper canine that should be saved, the cyst may first be opened to the mouth and allowed to shrink. Over months, the tooth may then erupt naturally into the arch, or be guided into position with orthodontic appliances.
Enucleation with preservation of the tooth, possible in some smaller lesions and where the tooth is in a favourable position.
Histopathological examination of the removed tissue is essential to confirm the diagnosis and rule out an OKC or ameloblastoma.
Bone grafting if a large defect remains after removal.
Long-term follow-up X-rays at intervals of 1, 2 and sometimes 5 years to confirm complete healing and rule out recurrence.
A patient-centred approach matters at every step, particularly for younger patients facing surgery for the first time. Honest discussion of why the cyst needs to come out, what the procedure involves, and how the tooth can be saved where possible is itself part of effective care, values that sit at the heart of our clinical philosophy.
What's the long-term outlook?
The outlook for a properly treated dentigerous cyst is excellent. Once the cyst has been enucleated or successfully decompressed, recurrence is uncommon. Where the involved tooth is saved, particularly an upper canine in a child, long-term function and appearance are generally very good. Where the involved tooth is removed (most often a wisdom tooth), the bone usually heals over months and the area returns to normal. Long-term review is recommended for the first few years to confirm the lesion has not recurred and to ensure the diagnosis was indeed a dentigerous cyst rather than a more aggressive lookalike.
A note on this article
This article is for educational purposes only and does not constitute a clinical diagnosis. Please consult a registered dental practitioner for assessment and treatment advice.
The cover image above is an AI-generated illustration based on the most common visible features of this condition described in clinical pathology references. It is not a photograph of a real case and should not be used to diagnose or rule out the condition in your own situation. If you are concerned about something you have noticed, please book an assessment with a registered dental practitioner.
References
Cawson, R. A., & Odell, E. W. (2017). Cawson's essentials of oral pathology and oral medicine (8th ed.). Elsevier. Chapter 7, Cysts of the Jaws: Dentigerous cysts with central, lateral and circumferential variants, enucleation (a minor surgical procedure where the cyst is removed cleanly from its bony cavity) and marsupialisation (a smaller first operation that opens the cyst and lets it shrink before definitive removal), pp. 121 to 123.
Neville, B. W., Damm, D. D., Allen, C. M., & Chi, A. C. (2023). Oral and maxillofacial pathology (5th ed.). Elsevier. Chapter 15, Odontogenic Cysts and Tumors: Dentigerous Cyst (Follicular Cyst) with detailed clinical, radiographic and histopathologic features, pp. 685 to 689.
Regezi, J. A., Sciubba, J. J., & Jordan, R. C. K. (2017). Oral pathology: Clinical pathologic correlations (7th ed.). Elsevier. Chapter 10, Cysts of the Jaws and Neck: Dentigerous cyst with developmental and inflammatory pathogenesis.
Frequently asked questions
What is a dentigerous cyst?
A dentigerous cyst is a fluid-filled sac that forms around the crown of an unerupted tooth, most commonly a lower wisdom tooth or upper canine. It is benign and usually painless but can grow large enough to displace teeth or weaken the jawbone if left untreated.
How is a dentigerous cyst found?
Most are discovered by chance on a routine dental X-ray, often a panoramic image. The classic appearance is a well-defined dark area attached to the neck of an unerupted tooth crown.
Is a dentigerous cyst dangerous?
It is benign, but it does keep growing and can cause bone thinning, tooth displacement, root resorption of neighbouring teeth and, very rarely, transformation into a more aggressive lesion. Surgical removal is the standard treatment.
How is it treated?
Treatment is surgical: enucleation (removal of the cyst with the involved tooth) or marsupialisation (opening and decompressing the cyst) when preserving an important tooth or avoiding nerve damage is preferred. Histopathology confirms the diagnosis after removal.



