Compiled from clinical pathology references. Medically reviewed by Dr Cristian Dunker, Principal Dentist, ArtSmiles Cosmetic Dentistry.
Quick summary
At a glance | Detail |
|---|---|
What it is | Developmental variations where some teeth fail to form (hypodontia) or extra teeth develop (hyperdontia). |
Who gets it | Hypodontia affects 3 to 10% of the population (excluding wisdom teeth); hyperdontia affects 1 to 3%. Both often run in families. |
Main cause | Strong genetic component, with possible contributions from trauma, infection, radiation, chemotherapy, and certain syndromes. |
What you might notice | A missing adult tooth, a retained baby tooth, an extra tooth (often between the upper central incisors), or delayed eruption of front teeth in childhood. |
How serious | 🟡 Not dangerous in itself, but affects bite, alignment, and eruption of other teeth. Coordinated long-term planning matters. |
Treatment | Monitoring, orthodontics, restorative work (fillings, bridges, or implants), and surgical removal of problem supernumerary teeth. |
What is it?
"Hypodontia" and "supernumerary teeth" are the two main developmental variations in the number of teeth. The textbooks use a few related terms:
Hypodontia, the failure of one to five teeth to develop.
Oligodontia, the failure of six or more teeth to develop, excluding the third molars.
Anodontia, the total absence of tooth development; very rare and typically part of a syndrome.
Hyperdontia, the development of an increased number of teeth; the extra teeth are called supernumerary teeth.
Mesiodens, the most common supernumerary tooth, which sits between the two upper central incisors.
Both missing and extra teeth are common enough that every dentist sees them regularly. They can affect bite, alignment, appearance and the eruption of normal teeth, and most cases benefit from a planned long-term approach.
Who tends to get it?
The textbooks describe a fairly recognisable profile:
Hypodontia affects 3 to 10% of the permanent dentition when third molars are excluded, rising to about 23% when third molars are included. There is a slight female predominance.
Most commonly missing teeth (after third molars) are the second premolars and the upper lateral incisors.
Least likely to be missing: the upper central incisors, the lower first molars and canines.
Hypodontia is uncommon in the deciduous (baby) dentition (less than 1%), but a missing baby tooth is a strong predictor of a missing successor.
Hyperdontia affects about 1 to 3% of the population, with a slight male predominance.
Most common supernumerary tooth: mesiodens, a small, often peg-shaped tooth between the upper central incisors.
Other common supernumerary locations: behind the upper third molars (paramolar or distomolar), and between the upper lateral incisor and canine.
Both can be associated with a wide range of syndromes. Neville lists more than 80 syndromes associated with tooth agenesis (failure of teeth to develop) and a similar list of syndromes associated with extra teeth.
Many cases are isolated (not part of any syndrome), often run in families, and follow a roughly autosomal dominant inheritance pattern with incomplete penetrance (meaning the family trait does not always show in every relative).
What causes it?
The textbooks describe a strong genetic component plus modest environmental influence:
Hypodontia genes, more than 200 genes are involved in tooth development. The most commonly implicated in nonsyndromic hypodontia are WNT10A, PAX9, MSX1 and AXIN2.
Hyperdontia genes, fewer specific genes have been linked, with RUNX2 (in cleidocranial dysplasia, a condition that affects bones and teeth) and APC (in Gardner syndrome, a condition that affects the bowel and teeth) the best known.
Environmental influences on hypodontia, trauma to the developing tooth bud, infection, radiation therapy, chemotherapy, endocrine disturbances, and severe nutritional deficiency.
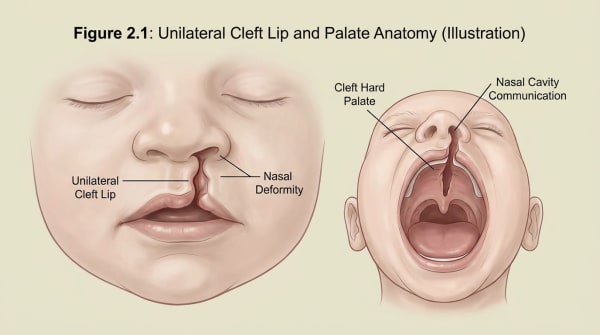
Cleft lip and palate significantly increases the risk of both missing and extra teeth in the cleft area. See Cleft Lip and Palate.
Idiopathic in many isolated cases, a single missing or extra tooth often occurs without any identifiable underlying cause.
How does it develop?
Tooth development requires the dental lamina (the strand of tissue that gives rise to all teeth) to send out signals at exactly the right times and locations. Hypodontia results when a part of this lamina fails to form, fails to send the signal, or is disrupted by genetic or environmental factors. Hyperdontia results when the lamina sends out an extra signal, producing an additional tooth bud.
Most teeth develop between the sixth week of pregnancy and the early teens. Any significant disruption during this window can affect the number, size or shape of the teeth that ultimately appear.
What might you notice?
What it looks like
Hypodontia:
An obvious gap where a tooth would normally be expected, particularly in the upper lateral incisor or second premolar position.
A retained baby tooth that has not been replaced because no adult tooth formed underneath.
A microdontic (small, often peg-shaped) tooth in place of an expected normal tooth (often the upper lateral incisor), sometimes a sign of partial tooth-formation failure.
Multiple missing teeth with crowded remaining teeth in oligodontia.
Hyperdontia:
A small extra tooth between the upper central incisors (mesiodens), sometimes visible in the mouth, sometimes hidden as an unerupted tooth on X-ray.
An extra wisdom tooth behind the third molar.
An extra tooth between the upper lateral incisor and canine.
A delayed eruption or rotation of a normal tooth caused by an unerupted supernumerary blocking its path. See Eruption Cyst for a related cause of delayed tooth appearance.
What it feels like
Most patients with hypodontia or supernumerary teeth have no symptoms beyond the anatomical variation. Symptoms when they occur may include:
A noticeable gap that affects appearance and self-confidence.
Difficulty eating in cases of multiple missing teeth.
Crowding or misalignment caused by extra teeth or by drift into space left by missing teeth.
Unerupted upper central incisor in young children with a buried mesiodens.
Late eruption of front teeth as a presenting feature of an unerupted supernumerary.
What an X-ray might show
X-rays are the gold standard for confirming both hypodontia and supernumerary teeth:
Panoramic X-rays show the full dentition and easily reveal missing or extra teeth.
Periapical X-rays are useful for confirming the location of an unerupted supernumerary.
Cone-beam CT (a 3D dental X-ray) is sometimes used for complex supernumerary teeth or when surgical removal is being planned.
Long-term tracking X-rays are often taken in childhood to monitor expected eruption timing and to spot supernumeraries before they cause problems.
What happens at the dentist?
Hypodontia or supernumerary teeth are most often picked up at a routine dental check-up and clean at ArtSmiles, often during childhood when an expected tooth has not erupted on time. The dentist will typically:
Examine the dentition carefully and compare it with the expected eruption sequence for the patient's age.
Take panoramic X-rays to confirm the number of teeth present and to identify any unerupted supernumeraries.
Take a careful history of family members with similar dental patterns, since these conditions often run in families.
Look for syndromic features that might suggest a wider underlying condition, particularly hypohidrotic ectodermal dysplasia (a syndrome affecting hair, sweat glands and teeth) for severe hypodontia, or cleidocranial dysplasia for severe hyperdontia.
Refer to an orthodontist for early advice on eruption timing, space management and long-term planning.
Refer to an oral surgeon for surgical removal of unerupted supernumeraries when indicated.
Plan a staged restorative pathway, particularly for adolescents and young adults with hypodontia approaching long-term restoration of missing teeth.
Is this serious?
🟡 Neither hypodontia nor hyperdontia is dangerous in itself. The reason both deserve attention is that they can affect bite, alignment, eruption of other teeth, and self-confidence, and these effects are often easier to manage if they are recognised early.
If your child has not developed an expected baby or adult tooth by the usual age, or if a routine X-ray has shown an extra tooth, it is worth booking an assessment so the right plan can be put in place.
Could it be something else?
Several situations can mimic missing or extra teeth. The textbooks list these as the main differentials:
Unerupted impacted teeth, the tooth is present but stuck under the gum or bone; X-ray distinguishes from true agenesis.
Ectopic eruption, the tooth is coming through in the wrong place rather than missing.
Retained primary teeth without a successor, common in localised hypodontia, often misread as a "fully present" dentition.
Ankylosis, fusion of the tooth root to the bone, often producing a tooth that looks "submerged" relative to its neighbours.
Recently extracted teeth, important to distinguish from teeth that never developed; the dentist's history-taking handles this.
Dens Invaginatus, a tooth that has folded in on itself during development, which can look like an extra structure on X-ray.
Amelogenesis Imperfecta, a developmental enamel disorder where small or peg-shaped teeth can mimic localised hypodontia.
How is it treated?
Treatment depends on the pattern and severity, the patient's age and the broader dental and aesthetic context.
Hypodontia:
Monitoring and timely orthodontic referral during childhood.
Maintaining the deciduous tooth as long as possible when no successor exists, often well into adulthood, since the baby tooth can serve a long time before requiring replacement.
Orthodontic space management, closing the space (with the canine moving forward) or opening it for future restoration, depending on the pattern.
Restoration with a dental filling to reshape a peg-shaped lateral incisor.
Resin-bonded bridges, conventional bridges or dental implants in adulthood for restoration of missing teeth.
Removable dentures in cases of severe oligodontia or anodontia, sometimes started in childhood for aesthetic and functional reasons.
Coordination with paediatric and medical specialists when severe hypodontia is part of a syndrome such as hypohidrotic ectodermal dysplasia.
Supernumerary teeth (hyperdontia):
Surgical removal of unerupted supernumeraries that are blocking eruption of normal teeth, particularly mesiodens preventing upper central incisors from coming through.
Monitoring of small, deep, asymptomatic supernumeraries that are not interfering with anything, sometimes the safer course.
Orthodontic management to align the dentition after removal.
Removal and restoration when the supernumerary has erupted into a visible position and is causing aesthetic or hygiene problems.
A patient-centred approach matters here, particularly with children. Parents often worry about appearance and timing, and a clear plan that explains what will happen, when, and why is itself part of effective care.
What's the long-term outlook?
The outlook is excellent. Children with hypodontia who are managed in a coordinated way with orthodontics and timely restoration usually grow up with an attractive, functional dentition. Adults with isolated hypodontia have many modern restorative options available, including resin-bonded bridges and implants, that produce excellent long-term results. Supernumerary teeth that are removed early rarely cause lasting problems, and small asymptomatic supernumeraries left in place are monitored across routine X-rays.
Where hypodontia or hyperdontia is part of a wider syndrome, the long-term plan is shaped by the broader medical picture, with the dental component contributing to overall quality of life and function.
A note on this article
This article is for educational purposes only and does not constitute a clinical diagnosis. Please consult a registered dental practitioner for assessment and treatment advice.
The cover image above is an AI-generated illustration based on the most common visible features of this condition described in clinical pathology references. It is not a photograph of a real case and should not be used to diagnose or rule out the condition in your own situation. If you are concerned about something you have noticed, please book an assessment with a registered dental practitioner.
References
Neville, B. W., Damm, D. D., Allen, C. M., & Chi, A. C. (2023). Oral and maxillofacial pathology (5th ed.). Elsevier. Chapter 2, Abnormalities of Teeth.
Cawson, R. A., & Odell, E. W. (2017). Cawson's essentials of oral pathology and oral medicine (8th ed.). Elsevier. Chapter 2, Disorders of Development of the Teeth.
Regezi, J. A., Sciubba, J. J., & Jordan, R. C. K. (2017). Oral pathology: Clinical pathologic correlations (7th ed.). Elsevier. Chapter on Abnormalities of Teeth.
Frequently asked questions
What is hypodontia?
Hypodontia is the developmental absence of one or a few teeth, where the tooth bud never formed in the jaw. The most commonly missing teeth (apart from wisdom teeth) are the upper lateral incisors and lower second premolars. Mild hypodontia affects up to around 5-10% of people.
What are supernumerary teeth?
Supernumerary teeth are extra teeth beyond the normal set of 20 baby or 32 adult teeth. The most common type is the 'mesiodens', a small conical extra tooth between the upper front incisors. Supernumerary teeth can stay buried in the bone, displace neighbouring teeth, or block their eruption.
How are missing or extra teeth managed?
Management depends on the number, position and the patient's age and preferences. Options include orthodontics to close the gaps, dental implants, bridges or partial dentures to replace missing teeth, and surgical removal of supernumerary teeth that are blocking eruption or crowding the bite. Coordination between general dentist, orthodontist and oral surgeon is the norm.
Do hypodontia and extra teeth run in families?
Yes, often. Both conditions have a recognised genetic component, so it is common to see other family members with the same pattern of missing or extra teeth. They are also more frequent in patients with cleft lip and palate and some other syndromes. A family-aware dental review helps catch issues early.