Compiled from clinical pathology references. Medically reviewed by Dr Cristian Dunker , Principal Dentist, ArtSmiles Cosmetic Dentistry.
Quick summary
Also called | Dens in dente, tooth-within-a-tooth, invaginated odontome (a non-cancerous tooth-like growth) |
How urgent? | 🟡 Worth assessing, not painful in itself but the deep pit can let bacteria reach the pulp early; preventive treatment can avoid future pulp infection |
Common or rare? | Reported prevalence ranges widely from 0.04% to 10% of patients depending on diagnostic criteria |
Who it affects | Most often the upper lateral incisors of children and young adults; can also affect upper central incisors, premolars, canines and molars |
Who treats it | General dentist for diagnosis and protective restoration; endodontist (a dentist who specialises in root canal treatment) if the pulp becomes infected |
Based on | Neville, with cross-references in Cawson and Regezi |
What is it?
Dens invaginatus is a developmental tooth defect in which the enamel of the tooth surface folds inward during development, creating a small enamel-lined pit, channel or sac inside the body of the tooth. The textbooks describe two main forms, coronal (in the crown), which is far more common, and radicular (in the root). On X-ray, the inverted fold gives the appearance of "a tooth within a tooth", which is where the older name dens in dente comes from. Although the lesion is usually painless, the deep enamel-lined pit can let bacteria reach the pulp very early in the tooth's life, sometimes producing pulp infection before the patient is even aware that anything is wrong with the tooth. Recognising and protecting these pits early can prevent that complication.
Who tends to get it?
The textbooks describe a fairly recognisable distribution:
Most often affects the upper lateral incisors, the small front teeth either side of the central incisors. Other commonly affected teeth, in decreasing order, are the upper central incisors, premolars, canines and molars.
Strong predilection for the upper jaw.
Children and young adults, usually picked up shortly after the tooth comes through.
Both sides of the mouth can be affected; bilateral lesions in the upper lateral incisors are well recognised.
Both sexes affected equally.
Genetic component, the condition can run in families, and is reported more often in some populations than others.
The reported prevalence varies widely, from as little as 0.04% to as much as 10% of patients, depending on how strictly the diagnosis is made and how thoroughly teeth are X-rayed.
What causes it?
The exact cause is unknown, but the textbooks describe several possible mechanisms:
Folding-in of the enamel organ during the developmental stage of tooth formation. The thin sheet of cells that forms the enamel folds inward, taking the future enamel surface with it.
A growth-pressure imbalance between the enamel organ and the surrounding tissue.
Inherited tendency, with some families showing the trait in multiple members.
Possibly related developmental anomalies, dens invaginatus is often associated with shovel-shaped incisors, talon cusps and dens evaginatus, suggesting a shared family of developmental tendencies.
There is no environmental cause. Diet, fluoride, infection during childhood and trauma do not produce dens invaginatus.
How does it develop?
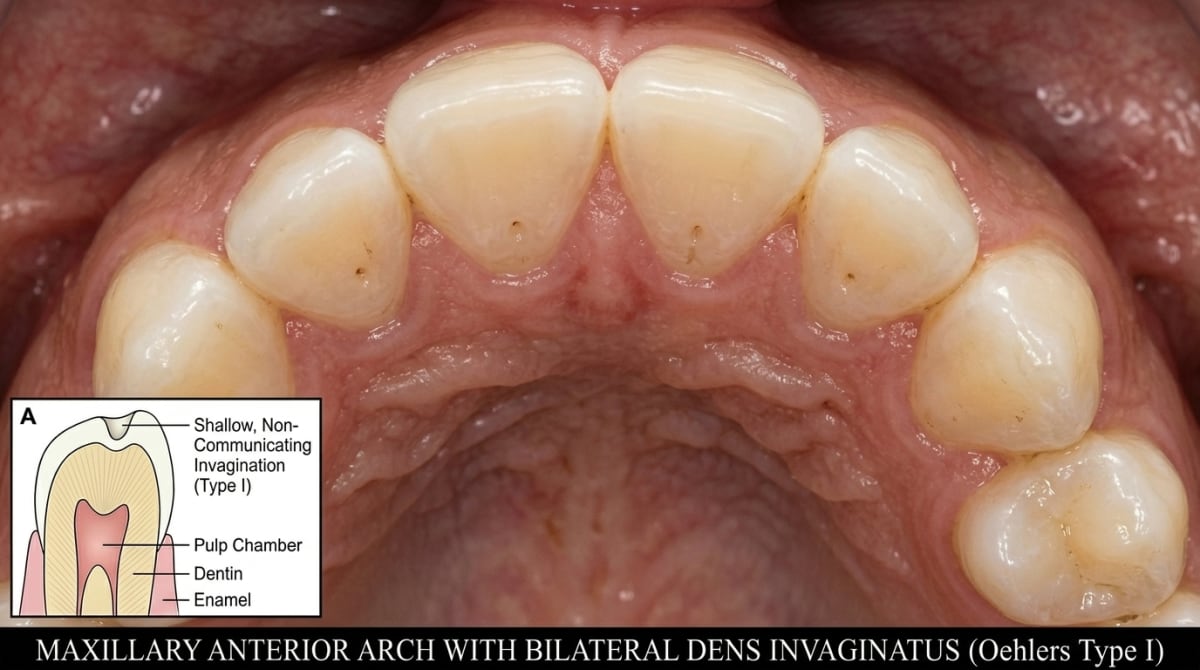
During tooth formation, the enamel organ should form a smooth surface that becomes the crown of the tooth. In dens invaginatus, part of this surface folds inward instead of outward. The folded part is still lined by enamel, so on the inside of the tooth there is a deep, enamel-lined pit. The textbooks describe three classic Oehlers types:
Type I, a small invagination (a small inward fold of enamel that forms a pit inside the tooth) confined to the crown, ending in a blind sac inside the enamel layer.
Type II, a deeper invagination that extends below the cementoenamel junction (the line where the enamel meets the root) and ends as a blind sac inside the root.
Type III, the invagination extends through the entire root and opens through the side of the root, sometimes producing a second "apex" on the lateral root surface.
Once the tooth comes through, the soft tissue that originally filled the invagination loses its blood supply, dies, and creates a tiny pocket where bacteria from the mouth can settle. Because the invagination's inner wall is often very close to the pulp, and sometimes communicates directly with it, bacteria can reach the pulp before the tooth is more than a few years old.
What might you notice?
What it looks like
The classic clinical findings include:
A small pit or groove on the back (palatal) surface of an upper lateral or central incisor.
A slightly bulbous or barrel-shaped tooth compared with its opposite side.
Sometimes a localised enlargement of the cingulum (the bump on the back of front teeth).
A deep coronal labial groove in some cases.
The invagination itself is not visible to the naked eye; the diagnosis is usually confirmed on X-ray.
What it feels like
Most cases of dens invaginatus produce no symptoms at all in early childhood. Symptoms when they appear typically reflect pulp infection rather than the invagination itself:
Pain or tenderness in the affected tooth, sometimes with no obvious cause.
Swelling of the gum near the tooth.
A small abscess (parulis) above the tooth.
Loose tooth in advanced cases.
No symptoms at all when the invagination has been protectively restored before bacteria reached the pulp.
The textbooks specifically note that dens invaginatus can produce pulp infection long before the apex has closed, meaning a young permanent tooth can lose its vitality (a test to check whether the nerve inside the tooth is still alive) before the patient is even aware of any problem.
What an X-ray might show
X-rays are the most reliable way to find dens invaginatus. Typical findings:
A deep, radiopaque enamel-lined pit projecting into the body of the tooth from the cingulum or palatal pit area.
A "tooth-within-a-tooth" appearance, particularly in Type II lesions.
A perforation through the lateral root surface in Type III.
Sometimes dystrophic enamel (poorly formed or weakened enamel) in the base of a dilated invagination.
Periapical changes if the pulp has become infected.
A small-volume CBCT (a 3D dental X-ray) scan is often invaluable for mapping the lesion before treatment.
What happens at the dentist?
Dens invaginatus is most often picked up at a routine dental check-up and clean at ArtSmiles, often when a child or young adult has X-rays for orthodontic assessment or other dental care. The dentist will typically:
Examine the upper front teeth carefully for a deep palatal pit, a bulbous shape, or any subtle indication of a coronal invagination.
Take periapical X-rays (close-up X-rays showing the whole length of a single tooth and the bone around its root) to confirm the presence of an enamel-lined invagination.
Order a small-volume CBCT scan in selected cases for detailed mapping, particularly for Types II and III.
Test the vitality of the affected tooth with cold or electric pulp testing.
Recommend protective restoration of the pit shortly after eruption to prevent later pulp infection.
Refer to an endodontist when the pulp has already become infected.
Is this serious?
🟡 The lesion itself is benign, but its proximity to the pulp means it carries a real risk of pulp infection, sometimes long before the patient suspects anything is wrong. With early protective restoration, this risk can be largely prevented. Once the pulp has become infected, the treatment is more complex but still usually successful.
If a routine X-ray has shown an unusual enamel fold inside an upper front tooth, it is worth booking an assessment so a protective filling or further treatment can be planned before any infection develops.
Could it be something else?
Several conditions can produce a similar clinical or radiographic picture. The textbooks list these as the main differentials:
Dens evaginatus, the opposite developmental defect, with an outward bump (talon cusp) rather than an inward fold. The two can occur in the same tooth.
Deep palatal pit without true invagination, a normal anatomical variation that is more shallow and not lined deep into the dentine by enamel.
Dental caries, a soft brown cavity in the same area can produce similar symptoms.
Periapical disease from another cause, including a previous knock to the tooth that died silently.
Dilated odontome, a more severe developmental anomaly resulting from extensive disturbance of tooth formation.
How is it treated?
Treatment depends on the type, the size of the invagination and whether the pulp has been infected.
At-home measures and habits:
Maintain excellent oral hygiene, particularly around the back of the upper front teeth where palatal pits collect plaque.
Use a soft-bristled toothbrush with gentle palatal strokes to clean the cingulum area.
Attend regular dental check-ups so any new periapical change can be picked up quickly.
Professional steps your dentist may consider:
Protective restoration of the pit with a small composite filling shortly after eruption, the most effective single intervention. Sealing the pit prevents bacteria from reaching the pulp.
Topical fluoride applications to strengthen the surrounding enamel.
Root canal treatment when the pulp has already become infected, often more complex than for an ordinary tooth because of the unusual internal anatomy. A small-volume CBCT scan and treatment by an endodontist are often advised.
Surgical management for Type III lesions perforating the root surface, sometimes combined with non-surgical root canal treatment of the main canal.
Extraction as a last resort when the tooth cannot be saved.
Long-term follow-up with X-rays to confirm the pulp remains healthy or that any treatment has been successful.
A patient-centred approach matters here. A young patient with an apparently healthy front tooth being told it needs a filling for "preventive" reasons can find the recommendation hard to follow without a clear explanation. Calm, unhurried discussion of what dens invaginatus is, why early protection matters, and how simple the protective treatment is is itself part of effective care, values that sit at the heart of our clinical philosophy.
What's the long-term outlook?
The outlook is excellent when dens invaginatus is identified and protectively restored early. Many patients live their entire life without ever needing more than a small composite filling at the affected pit. Where the pulp has already been involved, modern endodontic techniques, including bioceramic materials and microsurgical root canal treatment, give a good chance of saving the tooth. Type III lesions, with perforation of the root surface, can be more challenging but are also often manageable with combined endodontic and surgical care. Across all forms, regular dental review and timely action are the keys to a good long-term outcome.
A note on this article
This article is for educational purposes only and does not constitute a clinical diagnosis. Please consult a registered dental practitioner for assessment and treatment advice.
The cover image above is an AI-generated illustration based on the most common visible features of this condition described in clinical pathology references. It is not a photograph of a real case and should not be used to diagnose or rule out the condition in your own situation. If you are concerned about something you have noticed, please book an assessment with a registered dental practitioner.
References
Neville, B. W., Damm, D. D., Allen, C. M., & Chi, A. C. (2023). Oral and maxillofacial pathology (5th ed.). Elsevier. Chapter 2, Abnormalities of Teeth: Dens Invaginatus (Dens in Dente), with Oehlers Type I, II and III classification, prevalence and treatment, pp. 88 to 91.
Cawson, R. A., & Odell, E. W. (2017). Cawson's essentials of oral pathology and oral medicine (8th ed.). Elsevier. Chapter 2, Disorders of Development: cross-reference for dens invaginatus.
Regezi, J. A., Sciubba, J. J., & Jordan, R. C. K. (2017). Oral pathology: Clinical pathologic correlations (7th ed.). Elsevier. Chapter on Abnormalities of Teeth: cross-reference for dens invaginatus.
Frequently asked questions
What is dens invaginatus?
Dens invaginatus is a developmental anomaly in which the enamel of a tooth has folded inwards before eruption, forming a deep pit, channel or even a 'tooth within a tooth'. It is most often seen in upper lateral incisors. The fold creates an easy pathway for bacteria to reach the pulp, even in a brand new tooth.
Why is dens invaginatus a problem?
The deep enamel fold often communicates with the pulp tissue early on, so a tooth with dens invaginatus can become infected even before the patient notices anything is wrong. Without early sealing or treatment, the pulp may die, leading to an abscess in a young person with no obvious cavity.
How is dens invaginatus diagnosed?
It is usually discovered by chance on a routine dental X-ray, which shows the characteristic radio-opaque fold inside the tooth. Sometimes a small dimple is visible on the back of an upper front tooth on clinical examination. Cone-beam CT may be used to map complex cases before treatment.
How is dens invaginatus treated?
Simple cases can be sealed with composite resin or fluoride to block the pit and prevent infection. More complex cases need root canal treatment of the tooth or the invaginated portion. Early identification, often at a child's routine check-up, gives the best chance of saving the tooth before symptoms develop.