Compiled from clinical pathology references. Medically reviewed by Dr Cristian Dunker, Principal Dentist, ArtSmiles Cosmetic Dentistry.
Quick summary
Also called | Orofacial cleft, cleft lip with or without cleft palate (CL/P), cleft palate only (CPO) |
How urgent? | 🔴 Significant congenital condition needing a coordinated craniofacial team (a specialist team that cares for face, mouth and jaw conditions) from birth; long-term outcomes are excellent with timely care |
Common or rare? | Around 1 in 700 to 1 in 1,000 births in white populations; higher in some Asian and Native American groups |
Who it affects | Babies of any background; cleft lip with or without palate more common in boys, isolated cleft palate more common in girls |
Who treats it | A craniofacial team (paediatric surgeon, ENT, speech therapist, paediatric dentist, orthodontist, psychologist); family dentist supports everyday dental care |
Based on | Neville, Cawson, with cross-references in Regezi |
Cleft Lip and Cleft Palate
Cleft lip and cleft palate are among the most common differences a baby can be born with. They affect the upper lip, the roof of the mouth, or both, and they happen because parts of the face that normally fuse during early pregnancy do not quite meet. Today, with a coordinated care team and modern paediatric surgery, the great majority of children with a cleft grow up speaking, eating and smiling well.
What is it?
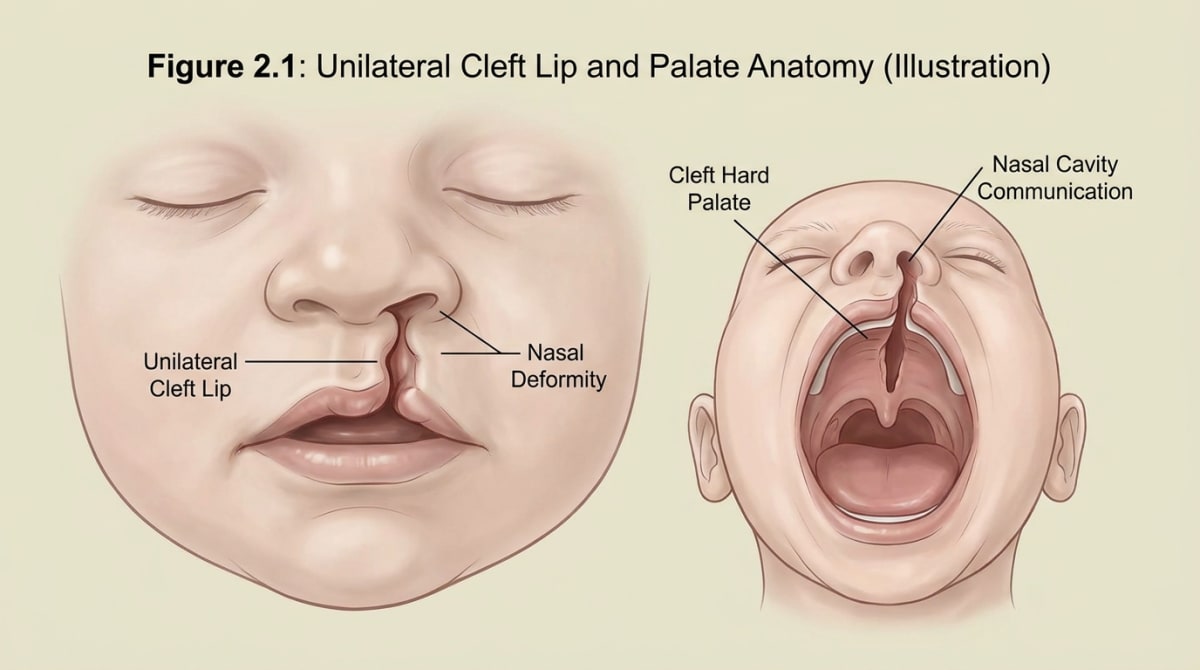
A cleft is a gap in tissue that should normally be joined. Cleft lip is a split in the upper lip; cleft palate is a split in the roof of the mouth. The two can occur together or separately:
Cleft lip with or without cleft palate (CL/P), about 45% of cases involve both lip and palate, and about 25% involve the lip alone.
Cleft palate only (CPO), accounts for around 30% of cases.
Cleft lip can be subtle or pronounced, and the textbook describes three forms: a microform (a small notch or scar in the lip), an incomplete cleft (a partial split that does not reach the nostril), and a complete cleft (a full split extending into the nostril).
About 80% of cleft lips are unilateral (one side only), and around 70% of those are on the left side. The remaining 20% are bilateral (on both sides), meaning a split on each side of the upper lip.
Who tends to get it?
Cleft lip and palate affect families across every background, but the chance varies between populations:
About 1 in 700 to 1 in 1,000 births in white populations.
Around 1.5 times higher in many Asian populations.
Up to 3.6 in 1,000 births in some Native American groups.
Around 0.4 in 1,000 in Black populations.
Cleft lip with or without cleft palate is more common in boys, while isolated cleft palate is more common in girls. Having a parent or sibling with a cleft increases the chance that another child in the family will have one.
What causes it?
In most cases the cause is multifactorial (caused by a mix of factors, not a single cause), a mix of inherited tendency and things that happen during the early weeks of pregnancy. Known contributors include:
Genetic factors. A family history of cleft raises the chance.
Maternal smoking. Smoking during pregnancy roughly doubles the risk.
Certain medicines. Phenytoin (an anti-seizure medicine) has been linked with up to a tenfold increase in risk; some other medicines also play a role.
Folic acid intake. Adequate folic acid before and during early pregnancy may help reduce the chance, which is why folate supplements are recommended for women planning a pregnancy.
Syndromes. A small proportion of clefts are part of a wider syndrome that includes other features.
A specific group worth mentioning is Pierre Robin sequence (a triad of small lower jaw, backward tongue and cleft palate), which combines cleft palate with a small lower jaw (micrognathia, a smaller-than-usual lower jaw) and a tongue that sits further back than usual (glossoptosis, a tongue that sits further back than usual). Babies with Pierre Robin sequence sometimes need extra support with breathing and feeding in the first weeks of life.
How does it develop?
The face forms very early in pregnancy. The lip and front of the palate are usually fused by about the seventh week, and the rest of the palate by about the twelfth week. If the developing tissues do not meet and join in time, a cleft remains.
The cleft is set before most parents even know they are pregnant. Nothing a parent did during the rest of pregnancy caused the cleft to appear later, and importantly, the cleft is not caused by anything the parent did or did not do during the birth itself.
What might you notice?
A cleft lip is usually visible at birth, and many are now identified on antenatal ultrasound (an ultrasound scan during pregnancy) during pregnancy. A cleft palate may be less obvious and is often picked up during the newborn examination, when a doctor or midwife checks the roof of the mouth.
Common things families and clinicians notice in the early weeks include:
Feeding differences. Babies with a cleft palate may struggle to create suction at the breast or with a standard bottle. Special bottles and teats designed for clefts usually solve this.
Milk coming through the nose. This happens because the mouth and nose are connected through the cleft, and it usually settles after palate repair.
A nasal-sounding cry or, later, speech. Air escapes through the nose because the palate cannot fully close off the airway.
Frequent ear infections and glue ear (fluid behind the eardrum), because the muscles that open the eustachian tubes (the small channels that connect the middle ear to the back of the throat) do not work as well when the palate is split.
Differences in tooth development in the area of the cleft, extra teeth, missing teeth, or teeth in unusual positions.
What happens at the dentist?
Children with a cleft usually have a craniofacial team that coordinates surgery, speech and hearing care. A general or paediatric dentist works alongside that team and supports the family with everyday dental care. At ArtSmiles, a typical visit involves:
A relaxed first visit. We let your child explore the chair and mirror at their own pace before any examination.
A gentle look at the teeth and gums, with extra attention to the area on either side of the cleft, where teeth are most often affected.
Personalised hygiene advice for the family, tooth-brushing techniques, fluoride toothpaste, and tips for cleaning around teeth that sit at unusual angles.
Early decay prevention. Children with a cleft are often more prone to tooth decay near the cleft because the area is harder to clean. We may recommend regular reviews, fluoride applications and dietary advice.
Coordination with the craniofacial team about the timing of orthodontic care and any dental procedures that need to fit around scheduled surgery.
We will never rush a child through a visit. If your child needs a little more time, we make space for that.
Is this serious?
A cleft is a significant difference, but it is not a disease and it is not life-threatening for most children. Modern paediatric surgery, speech therapy and orthodontic care mean that the long-term outcomes are excellent. Most adults with a history of cleft lip or palate live full, healthy lives.
Some areas do need ongoing attention through childhood:
Hearing. Glue ear is common in early childhood and may need ear tubes (grommets, tiny tubes placed in the eardrum to drain fluid).
Speech. Many children benefit from speech therapy after palate repair.
Teeth. Teeth near the cleft may need orthodontics or future replacement.
Facial growth. Surgery to repair the cleft can affect how the upper jaw grows, which is why orthodontic and sometimes jaw-surgery review continues into the late teens.
A timely, team-based approach helps each of these areas turn out well.
Could it be something else?
Some other conditions can look or sound similar to a cleft, especially when the cleft is subtle:
Submucous cleft palate (a hidden cleft under intact palate covering). The covering of the palate looks intact, but the muscle underneath is split. It is sometimes only noticed when speech develops or feeding is unusually difficult.
Bifid uvula (a split in the small fleshy projection at the back of the soft palate). The little fleshy projection at the back of the soft palate is split into two. On its own it is usually harmless, but it can be a sign of a hidden submucous cleft.
Pierre Robin sequence. As above, a combination of small lower jaw, backward tongue position and (often) cleft palate.
Lip pits or scars from healed lip injuries. These are sometimes mistaken for very mild cleft lip.
A craniofacial team or paediatric ENT specialist is best placed to tell these conditions apart. The dentist's role is to flag anything unusual and refer on when needed.
How is it treated?
Cleft care is a journey, not a single event. The exact timing varies between centres, but a typical Australian pathway looks like this:
Newborn period. Feeding support with specialised bottles, a paediatric review, and counselling for the family.
Around three months. Surgical repair of the cleft lip.
Before 18 months. Surgical repair of the cleft palate, timed to support speech development.
Early childhood. Hearing checks, speech therapy and routine paediatric dental care.
Around 8 to 11 years. Alveolar bone grafting (a small operation that places bone into the gum where the cleft was), where a small piece of bone is placed into the gum where the cleft was, to allow adult teeth to come through into a stable jaw.
Adolescence. Orthodontics to straighten the teeth, and sometimes a rhinoplasty (nose surgery) and jaw surgery to refine the final appearance and bite.
Adulthood. Ongoing dental care, with possible bridges, dental implants or other replacements for any teeth missing in the cleft area.
Throughout this journey, the family dentist plays a quiet but important role: keeping the remaining teeth healthy so that every other step has a strong foundation.
What's the long-term outlook?
The long-term outlook for a child born with cleft lip or palate is very encouraging. With timely surgery, speech therapy and dental care, most children grow up with confident speech, clear hearing, healthy teeth and a smile they feel proud of. Some will have a small scar on the lip and a slightly altered nostril shape; for many, that scar simply becomes part of their story.
The best outcomes come from steady teamwork between the family, the craniofacial team and the family dentist. At ArtSmiles, we are honoured to be part of that team for the families who choose us, and we are happy to coordinate with your child's craniofacial centre at any age.
A note on this article
This article is for educational purposes only and does not constitute a clinical diagnosis. Please consult a registered dental practitioner for assessment and treatment advice.
The cover image above is an AI-generated illustration based on the most common visible features of this condition described in clinical pathology references. It is not a photograph of a real case and should not be used to diagnose or rule out the condition in your own situation. If you are concerned about something you have noticed, please book an assessment with a registered dental practitioner.
References
Neville, B. W., Damm, D. D., Allen, C. M., & Chi, A. C. (2016). Oral and maxillofacial pathology (4th ed., Ch. 1: Developmental Defects of the Oral and Maxillofacial Region, Orofacial Clefts, pp. 1 to 7). Elsevier.
Cawson, R. A., & Odell, E. W. (2017). Cawson's essentials of oral pathology and oral medicine (8th ed., Ch. 2). Elsevier.
Regezi, J. A., Sciubba, J. J., & Jordan, R. C. K. (2017). Oral pathology: clinical pathologic correlations (7th ed.). Elsevier.
Frequently asked questions
What causes cleft lip and palate?
Most cases arise from a combination of inherited (genetic) susceptibility and environmental factors during the first 6-12 weeks of pregnancy, when the lip and palate form. Recognised influences include some medications, smoking, alcohol, folate deficiency and rare genetic syndromes. Often no clear single cause is identified.
When is cleft lip and palate repaired?
In Australia, primary surgical repair of a cleft lip is typically done around 3-6 months of age, and palate repair around 9-12 months, by a specialist cleft team. Further surgical, dental, speech and orthodontic care continues through childhood and adolescence as the face and teeth develop.
How does cleft lip or palate affect teeth?
Children with cleft often have missing or extra teeth in the cleft area (most commonly missing or malformed upper lateral incisors), delayed eruption, and crowded or rotated teeth. They benefit from early dental review, orthodontic planning, and sometimes implant or bridge work later to replace missing teeth.
Where do families get cleft care in Australia?
Cleft care in Australia is delivered through specialist multidisciplinary cleft and craniofacial teams based in major children's hospitals. Families typically see a coordinated team including paediatric surgeons, plastic surgeons, ENT surgeons, orthodontists, paediatric dentists, speech pathologists and psychologists. Your GP or paediatrician can arrange referral.