Living with a loose partial denture can be frustrating. It moves when you eat, it affects how you speak, and over time it can make you feel self conscious about your smile. When gum disease is also part of the picture, the situation becomes even more complex. This clinical case shares how we helped a patient move from a failing upper partial denture and damaged teeth to a strong, fixed smile using dental implants and zirconia bridge.
In this article
The Patient's Concerns
This patient came to ArtSmiles with two main complaints: poor aesthetics and a loose upper partial denture that was no longer functioning well. She was unhappy with the appearance of her smile and struggled with everyday tasks like eating.
Research consistently shows that patients with removable dentures report lower satisfaction and quality of life compared to those with fixed implant supported restorations. A 2023 systematic review by Abou-Ayash et al. (2023) found a strong positive effect on patient reported outcomes when edentulous patients were rehabilitated with implant supported fixed prostheses, particularly for those seeking stability and confidence in their smile.
Clinical Examination
A thorough examination revealed several findings:
Upper Arch
Gum disease (periodontitis) affecting the remaining upper teeth
Multiple upper teeth that were unrestorable due to the extent of decay and bone loss
The existing partial denture was poorly fitting and no longer providing adequate support
Lower Arch
Several teeth requiring fillings
One tooth needing root canal treatment
A deep clean to address gum health
One tooth requiring a crown
One tooth requiring extraction
Treating gum disease before implant placement is essential. A systematic review by Sousa et al. (2016) showed that patients with a history of periodontitis have higher rates of biological complications around implants, making it critical to stabilise periodontal health before proceeding with any implant rehabilitation.

The Treatment Plan
I designed a staged treatment plan that addressed both arches in a logical order:
Treat the gum disease first to create a healthy foundation
Complete the lower arch work (fillings, root canal, deep clean, and crown)
Extract the unrestorable upper teeth and place four dental implants
Provide 3D printed temporary teeth so the patient would never be without a smile
Refine the temporaries over multiple stages for the best possible aesthetics and bite
Install the final zirconia bridge with titanium bar after implant integration
Stage 1: Treating the Foundation
Before any implant work could begin, the gum disease needed to be brought under control. This involved deep cleaning and careful management of the periodontal condition. At the same time, the lower arch was restored with the necessary fillings, root canal treatment, and a crown to ensure the entire mouth was healthy and functional.
This step is often overlooked, but it is one of the most important. A 2022 systematic review by Tomasi et al. (2022) evaluated full arch fixed prostheses in patients with stage IV periodontitis and found that long term success depends heavily on thorough periodontal treatment before and after rehabilitation.
Try Smile Studio
Curious how a new smile might look on you before you commit to anything? Try Smile Studio, our free online tool. Upload a photo of your smile and preview different tooth shapes and shades right in your browser, in your own time and with no pressure. It works best on a computer or laptop, so open it on a desktop rather than your phone for the easiest experience. It is a simple way to explore the look you are after and bring those ideas to your consultation, so we can talk through what is realistic for your teeth. Keep in mind it is a visual guide to spark the conversation, not a treatment plan or a promise of results.
Stage 2: Implant Placement and Temporary Teeth
Once the gum disease was under control, we moved forward with the upper arch. The remaining unrestorable teeth were extracted and four dental implants were placed in the same appointment.
Placing implants at the time of extraction is a well supported approach. A 2025 clinical study by Sethi et al. (2025) evaluated immediately loaded implants placed in extraction sites using the All on 4 protocol and reported a 100% implant survival rate over two years, with comparable bone levels to implants placed in healed sites.
To make sure the patient had temporary teeth in only 24 hours, we designed and fabricated temporary bridges using 3D printed resin. These provisional restorations gave the patient a functional and aesthetic smile while the implants healed and integrated with the bone.
Over the following months, we created three sets of temporary bridges. Each set was refined based on the patient's feedback and our clinical assessment, progressively improving the aesthetics, bite relationship, and overall comfort. This iterative approach is one of the great advantages of digital workflows in implant dentistry, as highlighted by research from Papaspyridakos et al. (2023), which demonstrated that digitally fabricated prosthesis prototypes can achieve clinically acceptable fit through a complete digital process.

First temporary bridge showing teeth positioned too forward, making the smile unnatural. We also can see the smile slightly tilted. This is the reason why we execute multiple temporaries, to achieve the best aesthetics for each case, before executing the final bridge.
Stage 3: The Final Zirconia Bridge
After six months of healing and refinement through the temporary phase, the implants were fully integrated and the ideal aesthetics and bite had been established. We then fabricated and installed the final zirconia bridge with a titanium bar.
Zirconia was chosen for its proven durability and superior oral health outcomes. Long term research by Barootchi et al. (2020) showed that zirconia implant supported prostheses have a significantly higher survival rate (93.7% at five years) compared to metal acrylic alternatives (83%), with fewer complications and better long term value.
For patients with a history of gum disease, zirconia offers an additional benefit. Studies show that zirconia surfaces accumulate less plaque than acrylic, which is particularly important for patients who need to maintain excellent oral hygiene to protect their implants. A two year study by Cappare et al. (2021) confirmed significantly lower plaque accumulation around monolithic zirconia prostheses compared to metal acrylic ones.
The Result
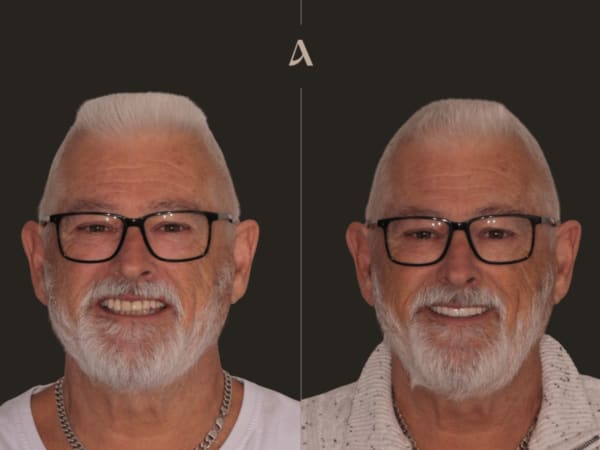
The transformation was remarkable. This patient went from a loose, uncomfortable partial denture and teeth affected by gum disease to a fully fixed, permanent smile. The upper arch now has a beautiful zirconia bridge supported by four implants, while the lower arch has been fully restored with quality restorations.
The patient can eat comfortably, smile with confidence, and maintain their oral health with regular hygiene visits as part of our maintenance program.

Before and after all on x with zirconia bridge
Why a Staged Approach Matters
This case highlights the importance of treating the whole mouth, not just the area of complaint. By addressing the gum disease first, completing the lower arch restorations, and then carefully planning the implant rehabilitation with multiple rounds of temporary bridges, we achieved a result that is built to last.
Key factors that contributed to the success of this case:
Gum disease treatment first: Creating a healthy foundation before placing implants
Full mouth approach: Restoring the lower arch alongside the upper for balanced function
3D printed temporaries: Three sets of provisional bridges allowed us to perfect the aesthetics and bite before committing to the final restoration
Zirconia with titanium bar: A material combination that offers strength, natural aesthetics, and better plaque resistance for a patient with a periodontal history
Six month healing period: Allowing adequate time for implant integration before the final bridge
If you are struggling with a loose denture, missing teeth, or gum disease and want to explore your options for a permanent solution, our team at ArtSmiles is here to help. Book a consultation to find out what is possible for your smile.
Disclaimer
This article documents one patient’s treatment at ArtSmiles. It is shared for educational purposes with the patient’s written consent. Individual results vary and depend on factors including oral health, bone and gum condition, general medical history, and how well the restoration is maintained after treatment. Nothing in this article is a guarantee of outcome, a substitute for a clinical examination, or advice specific to your case. Any treatment carries risks and potential complications, which will be explained to you at consultation.
Case executed by Dr Cristian Dunker
General Dentist
AHPRA DEN0002257085
ArtSmiles, Southport, Gold Coast
Frequently Asked Questions
Can you get All on 4 or All on X if you have gum disease?
Yes, but the gum disease has to be treated first. Active periodontitis is stabilised with a deep clean and, if needed, extractions of the unrestorable teeth. Once the gums are healthy, implant placement becomes predictable. Sousa et al. (2016) reported that patients with a history of periodontitis can still achieve good implant outcomes provided periodontal therapy is completed and maintained before implants are placed.
Can you have teeth the same day as the implants?
For most full-arch cases, yes. In this case we extracted the failing upper teeth and placed four implants in the same appointment, then delivered a 3D-printed temporary bridge within 24 hours. Sethi et al. (2025) reported 100% implant survival at two years using the same immediate-load All on 4 protocol in extraction sites.
Why use three sets of temporary bridges instead of one?
Because the first temporary rarely nails the final aesthetics and bite. With three iterations we adjusted tooth position, smile line, and bite relationship based on how the patient actually looked and chewed in real life, then locked the final design into zirconia. It adds time, but it avoids fitting a permanent bridge that looks wrong.
Why zirconia instead of an acrylic bridge?
Zirconia is harder to stain, collects less plaque, and lasts longer. Barootchi et al. (2020) reported 93.7% survival of zirconia full-arch prostheses at five years, compared to 83% for metal-acrylic. For a patient with a periodontal history, the plaque resistance is the real win, it protects the implants long term.
How long does the whole treatment take?
For this case, around 6 to 9 months from first consultation to final zirconia bridge. Gum disease treatment and lower-arch restorations take the first few weeks, implant surgery is one appointment, and the implants need around 6 months to fuse with the bone before the final bridge is fitted. The temporary bridge phase runs in parallel.
Written by Dr Cristian Dunker, BDSc, MBA.
Medically reviewed by Dr Cristian Dunker.
References
Abou-Ayash et al. (2023). Treatment effect of implant-supported fixed complete dentures and implant overdentures on patient-reported outcomes. Clin Oral Implants Res. PubMed
Sousa et al. (2016). A systematic review of implant outcomes in treated periodontitis patients. Clin Oral Implants Res. PubMed
Tomasi et al. (2022). Efficacy of rehabilitation of stage IV periodontitis patients with full-arch fixed prostheses. J Clin Periodontol. PubMed
Sethi et al. (2025). Immediately loaded full-arch prosthesis in extraction and healed sites using All-on-4/All-on-6. J Indian Prosthodont Soc. PubMed
Papaspyridakos et al. (2023). Complete digital workflow for prosthesis prototype fabrication with double digital scanning. J Prosthodont. PubMed
Barootchi et al. (2020). Long-term clinical outcomes and cost-effectiveness of full-arch implant-supported zirconia-based and metal-acrylic fixed dental prostheses. Int J Oral Maxillofac Implants. PubMed
Cappare et al. (2021). Implant rehabilitation of edentulous jaws with predominantly monolithic zirconia compared to metal-acrylic prostheses. J Biol Regul Homeost Agents. PubMed